
What Every Pharmacist Should Know about Breast Cancer: Part 2
Steph’s Note: Welcome back to Breast Cancer 101! If you haven’t read Clarissa’s Part 1 about breast cancer, you can do so here. I highly recommend it to understand the building blocks of how we decide on treatment before moving on to this article. This week, we will talk about systemic therapy because we are pharmacists, and this is where we thrive. Are your pharmacist neurons getting excited yet??
Quick recap: When it comes to treatment there are two big questions:
Where is the cancer?
What is the cancer?
To discuss treatment, we need to start with Question #1 and split breast cancer into two big broad categories. There’s early stage, and there’s advanced/metastatic stage. (Now technically, there is a whole spectrum in between these two, but because this is tl;dr, we’re simplifying it to these two categories. You’re welcome.)
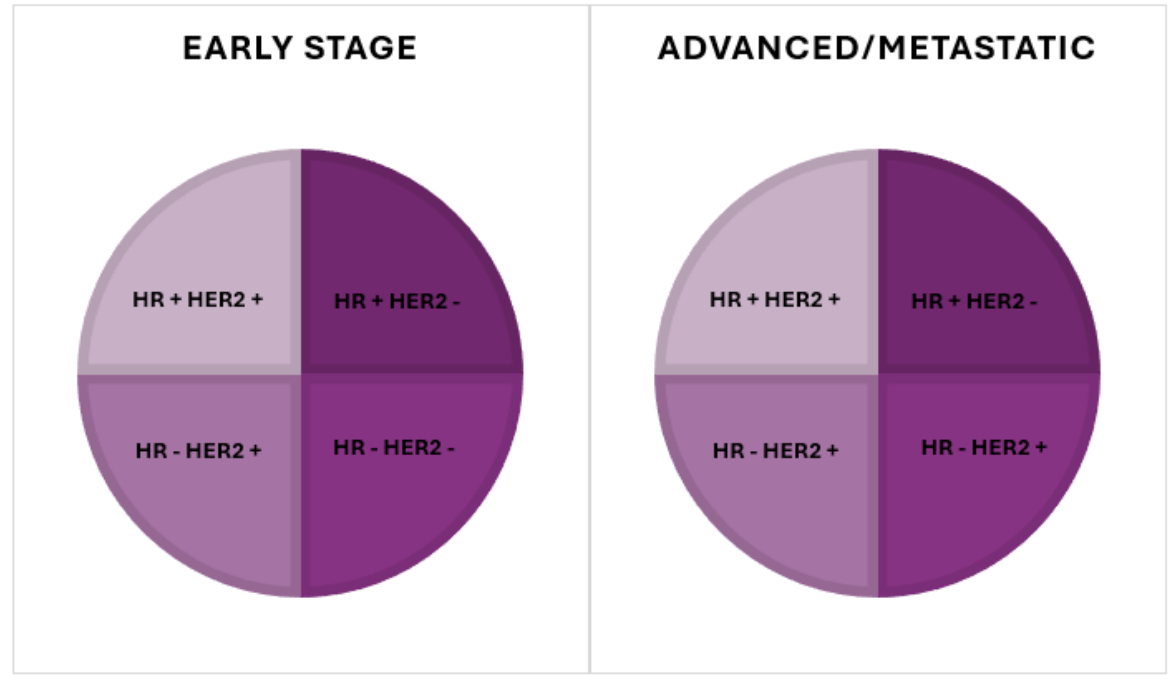
Then, within each of these big buckets, we have 4 smaller buckets that separate hormone receptor (HR) status and HER2 status, which is positive (+) or negative (-).
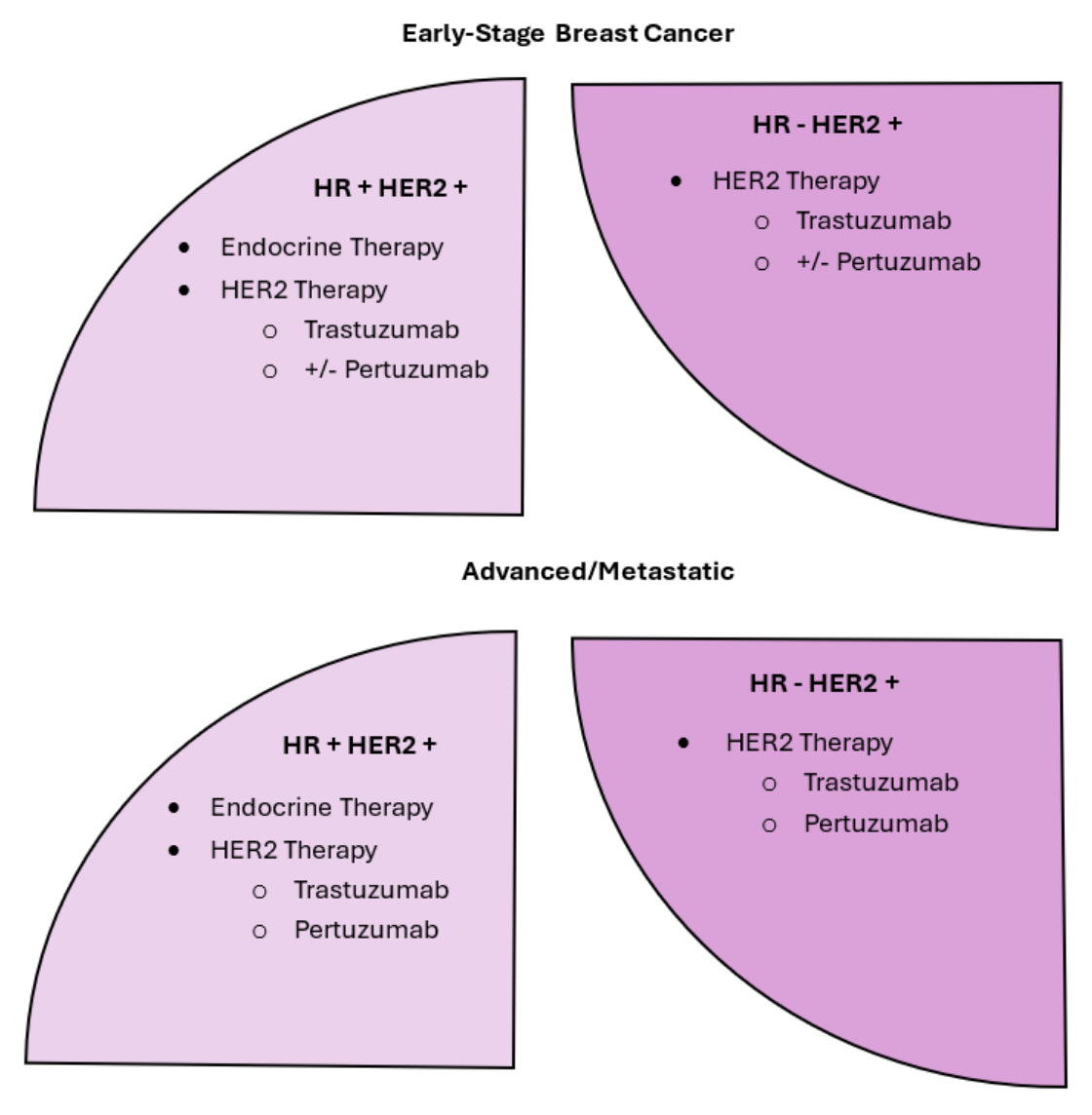
I have been working in oncology for years, and even while writing this, I had to draw the above image on a napkin for my visual self to keep everything organized. (There’s more to fill in these circles later.) (Image) To keep this from getting too long for tl;dr, we are going to focus mainly on common first line therapies. We are going to start with the medications we use to treat specific receptors, beginning with HR-positive.
Hormones, Hormones, Hormones
The most common type of treatment for hormone receptor positive breast cancer is, you guessed it, blocking those hormones from feeding the cancer! In early-stage breast cancer, these are usually given after surgery/radiation in order to prevent the cancer from coming back. In advanced or metastatic breast cancer, these are used in combination with other medications to help shrink and stop the growth of the cancer by cutting off its fuel source.
You’ll typically hear this called endocrine therapy.
An important distinction on how we treat patients with hormones is their menopausal status. Are they pre- or post-menopausal? Why is this important?
Depending on what their menopausal status is, estrogen can be coming primarily from different places. In pre-menopausal women, most of the estrogen is produced in the ovaries with some also coming from peripheral sources, such as adipose tissue (which is why obesity is a risk factor – higher body fat equals higher estrogen levels) and adrenal glands.
In post-menopausal women, estrogen production essentially stops in the ovaries, and the body relies on peripheral estrogen. So, this is why the menopausal status helps guide our therapy choices. (Image)
Now before we dig in, remember this: if the cancer doesn’t have hormone receptors, using a drug that blocks hormones is basically like trying to starve a vegetarian by telling them they can’t have meat. It’s not going to change a thing. Cutting hormones out of a cancer’s diet is only going to kill the cancer if the cancer relies on it to grow in the first place. But if it does, we have some excellent options for treatment.
Selective Estrogen Receptor Modulators (SERMs)
These medications bind to estrogen receptors in the body, but instead of a simple "on" or "off," they act as either estrogen-like agonists or antagonists depending on the specific tissue. This leads to tissue-selective effects like blocking breast cancer growth while boosting bone strength.
Tamoxifen is the medication we use in this class. It is recommended in pre- or perimenopausal women and is most commonly used in the early-stage setting. Although not the preferred first-line choice, it can also be used in postmenopausal women and in the advanced/metastatic setting.
It is generally taken for at least 5 years but can be taken for up to 10 years. Its most common side effects include hot flashes, increased vaginal discharge, and fluid retention.
*Important Counseling Tip*: It has a black box warning for increased risk of uterine cancer, stroke, and blood clots.
Aromatase Inhibitors (AIs)
These meds block the aromatase enzyme, which normally converts androgens (like testosterone) into estrogens (like estradiol). Therefore, by blocking this enzyme, these meds significantly reduce estrogen levels circulating in the blood. These work great in postmenopausal women where peripheral tissues produce the most estrogen. In pre-menopausal women, who still get estrogen from their ovaries, they would also either need to:
1. Be on ovarian suppression therapy with GnRH agonists (so that we are making sure to cut off estrogen from all sources – more on this in a bit), OR
2. Have an oophorectomy (a surgery which removes the ovaries and with them, their estrogen supply).

We have three aromatase inhibitors that are used:
Anastrozole (Arimidex)
Letrozole (Femara)
Exemestane (Aromasin)
Anastrozole and letrozole are typically preferred over exemestane in a first line setting due to better efficacy with fewer side effects. (Image) The most common side effects are fatigue, hot flashes, and muscle or joint aches and pains (similar to symptoms of menopause since we are cutting out estrogen). These are generally taken for at least 5 years and can be given up to 10 years in some patients.
Gonadotropin-Releasing Hormone (GnRH) Agonists
These are synthetic hormones that stimulate the GnRH receptors. Which you may think – don’t we want the opposite of that?
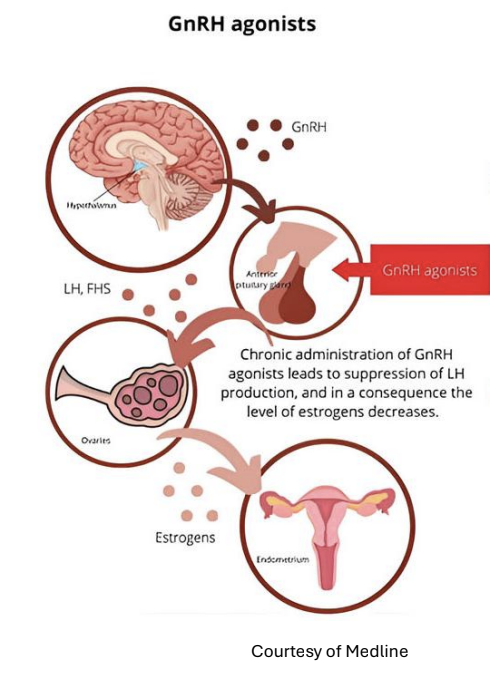
Yes. Yes, we do. Sorta.
Over time, this stimulation leads to long term desensitization and slowing down of the receptors, leading to the suppression of estrogen. (Image) As I mentioned above, we use these medications in pre-menopausal women on aromatase inhibitors to cut off estrogen coming from the ovaries.
Leuprolide (an intramuscular injection)
Goserelin (a subcutaneous injection)
As you can also imagine, these have similar side effects to the previous medications, since we are lowering estrogen. We commonly see hot flashes and headaches, along with some injection site pain since these are injectable.
CDK 4/6 Inhibitors
These nifty drugs work by inhibiting CDK4 and CDK6 (as you could have guessed by the name) in the cell cycle. They’re used in HR+ breast cancer because estrogen signaling directly triggers the CDK4/6 pathway, driving cell division. We use them along with endocrine therapy to prevent recurrence in early-stage breast cancer or to inhibit growth of the cancer in late-stage breast cancer.
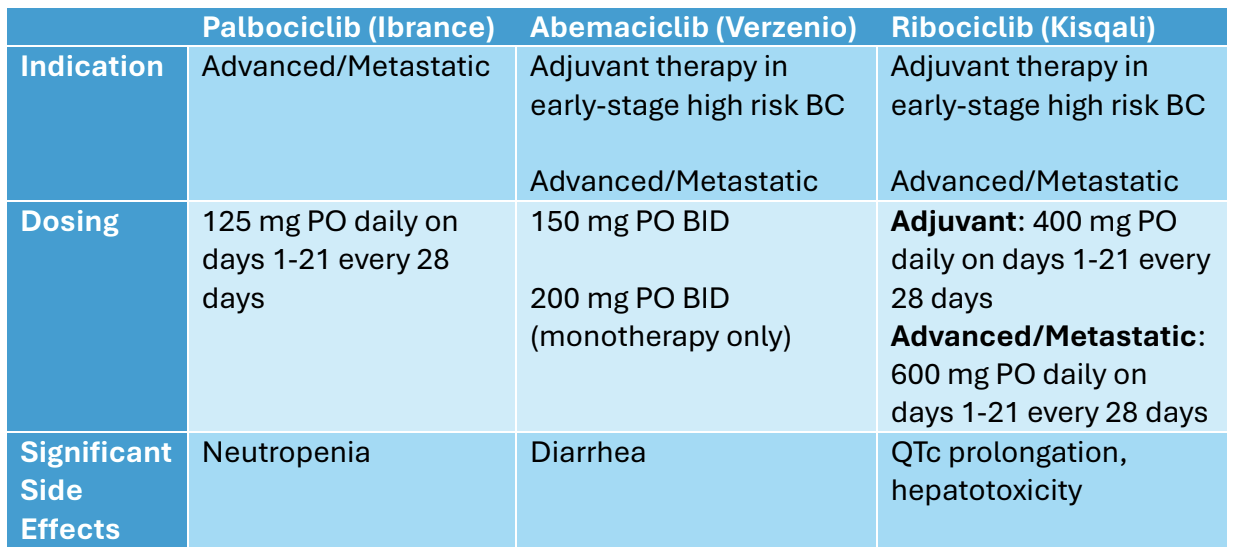
We have three CDK 4/6 Inhibitors to consider, and they each have their own pros and cons.
They are all indicated as preferred 1st line therapy for advanced/metastatic disease along with endocrine therapy; however, ribociclib holds the category 1 recommendation in the NCCN guidelines (Category 1 means it has high-level evidence that supports its use). (Image)
Abemaciclib and ribociclib are also indicated for early-stage high risk disease to prevent recurrence, each with their own set of criteria depending on the risk features.
They all share some side effects while also having some significant differences to consider when choosing one for your patients. The most common side effects include nausea, increased risk of infection, anemia, liver changes, skin rash, and diarrhea. They can also cause hair thinning or hair loss.
Ribociclib (Kisqali)
Ribociclib is currently approved for both early-stage high risk and advanced/metastatic disease. Of note, when given in early-stage high risk breast cancer, we dose it at a slightly lower dose than we do for advanced/metastatic.
One difference with this medication compared to its sister drugs is that it can cause QTc prolongation and therefore requires EKG monitoring prior to starting therapy, 2 weeks after starting therapy, and then as clinically indicated. It is also more likely than its counterparts to cause hepatotoxicity, so monitoring those liver enzymes is very important.
Abemaciclib (Verzenio)
Abemaciclib is also currently approved for both early-stage high risk and advanced/metastatic disease and has the same dosing in both settings. Its biggest side effect is diarrhea, and you may be thinking, “Oh that’s not so bad. Diarrhea is manageable…”

But the diarrhea with abemaciclib is no joke. (Image)
I have had several patients unable to leave their house due to the severity of diarrhea with this medication. As a counseling tip, I always recommend the patient have some loperamide on hand. And although we love our friend loperamide, sometimes it just doesn’t cut it, and patients need the abemaciclib dose-reduced. Luckily the data shows that the medication is just as effective at lower doses, with some providers opting to start lower and titrate up.
Of note, it is FDA approved to be used without endocrine therapy at a higher dose in the metastatic setting after progression on other therapies; however, this is less commonly used.
Palbociclib (Ibrance)
Palbociclib was the first of the CDK 4/6 inhibitors to come to market. It is currently approved for advanced/metastatic disease only, as the clinical trials in the early-stage setting did not show significant improvement. Its trademark side effect is that it can cause some pretty bad neutropenia, and this requires close monitoring.
Overview of CDK 4/6 Inhibitors
Alright, so where are we with all this? Let’s bring back up my napkin diagram.
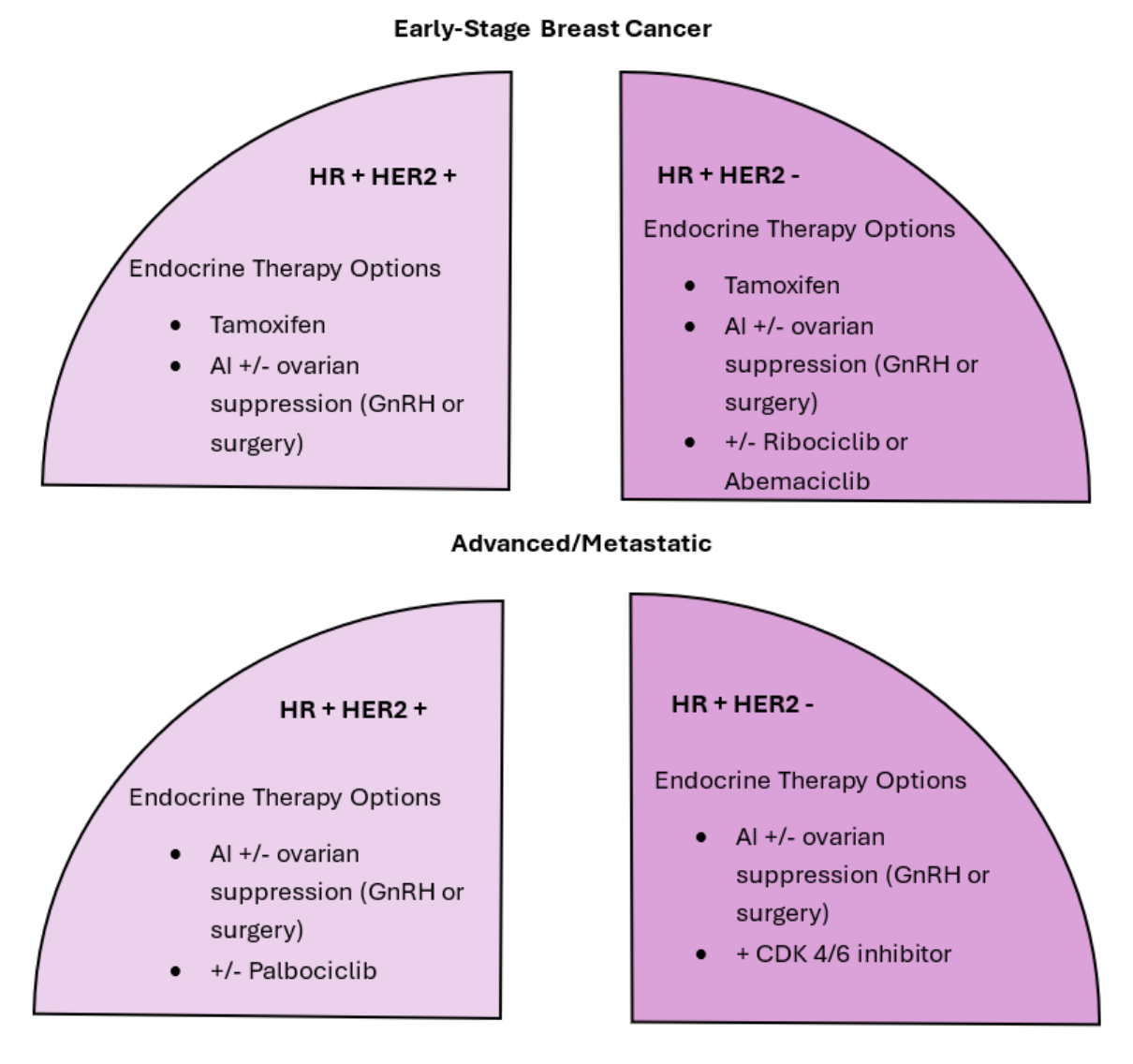
As we continue to fill the napkin diagram out, we will start seeing more differences. But for now, we can so far see where we use endocrine therapy and CDK4/6 inhibitors.
HER2 Targeting Agents
As we mentioned before, HER2 proteins are overly expressed on some cancer cells, making them HER2 positive. This protein promotes cell growth and tends to be more aggressive than other types of breast cancer. The good news with most cancers is that if it has an overexpression of something, we can target that.
We have two major workhorses in this area:
Trastuzumab (Herceptin)
Pertuzumab (Perjeta)
Trastuzumab is generally given as a part of all HER2 + breast cancer therapy, while pertuzumab is typically added for higher-risk disease, such as lymph node involvement or larger tumors. We also have a dark horse in this race, trastuzumab deruxtecan (Enhertu) – an antibody drug conjugate.
An important thing to know about anti-HER2 therapy is that inhibiting HER2 can also disrupt cardiac cells and lead to cardiac dysfunction. It’s recommended to get a baseline echocardiogram (aka, an echo), as well as every 3 months during treatment, and every 6 months after treatment is complete for up to 2 years to monitor left ventricular ejection fraction (LVEF).
BONUS LESSON 101: What is an antibody drug conjugate (ADC)?
I know you didn’t ask for it, but it’s really cool so I’m going to tell you. It’s a type of targeted cancer therapy comprised of 3 components. You have the monoclonal antibody that recognizes and binds to a specific antigen that’s expressed on tumor cells. Then you have the “payload,” which is a potent chemotherapy agent that’s attached to the antibody that gets directly deposited into the tumor cell. And then you have the linker, which connects the two together. (Image)
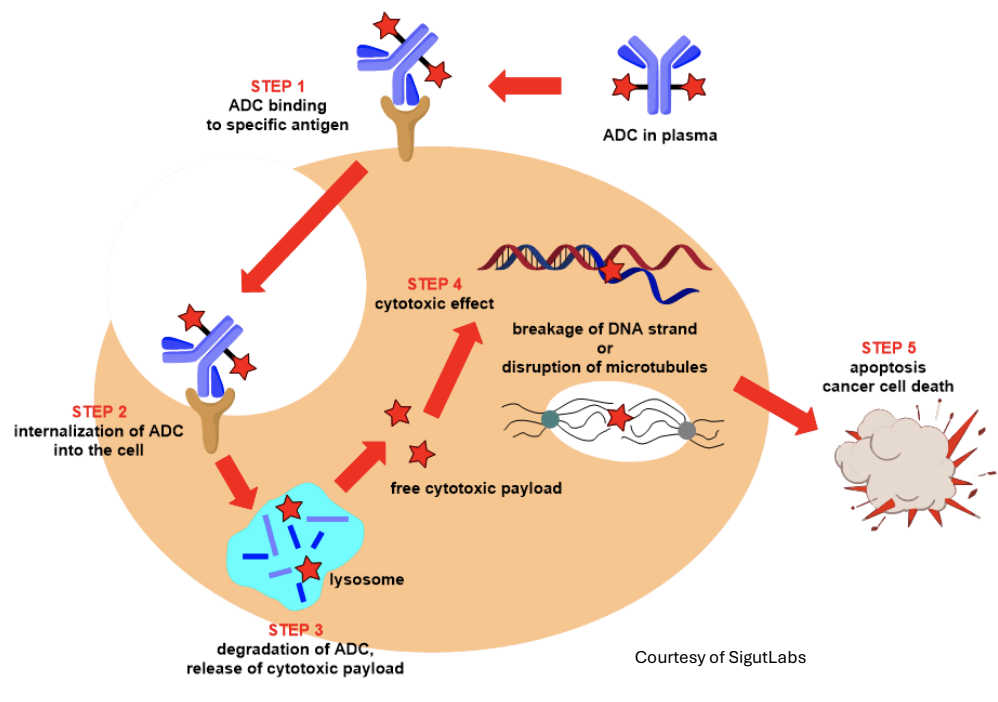
(Store this in the back of your brain because currently there are over 300 ADCs in development!)
Okay, so you know what we need now. Our handy dandy – Napkin Diagram! (I’m a 90s kid okay - where are my Blue’s Clues fans?) Let’s add in this new information!
Last but not least – chemotherapy (with a splash of immunotherapy)…
Chemotherapy (and Immunotherapy)
Chemotherapy can be used with any of the above options, as well as with immunotherapy, in patients with triple negative breast cancer (TNBC). The most common agents we see in the breast cancer world are:
Taxanes (Paclitaxel/Docetaxel)
These work by locking the cell’s internal “skeleton” (called microtubules) in place, which cancer cells need to divide. When the cells can’t divide normally, they stop growing and eventually die. This makes these drugs especially helpful against fast-growing breast cancer cells.
Side effects of note include low blood counts (white blood cells, red blood cells, and platelets), hair loss, neuropathy (nerve problems), and allergic-type reactions.
Carboplatin
Carboplatin works by binding to DNA in cancer cells, which prevents the cells from copying their DNA and dividing. This leads to cancer cell death.
Side effects include low blood counts, kidney toxicity, and neuropathy.
Doxorubicin
This works by damaging cancer cell DNA and stopping the cells from making new DNA, which prevents them from dividing and leads to cell death. Because breast cancer cells divide quickly, they are especially sensitive to this kind of damage.

When I say red urine with doxorubicin, I mean raspberry red urine.
Side effects include low blood counts, hair loss, mouth sores, and red/orange urine (or other secretions like tears!) for 2-3 days after treatment.
(Harmless! But creepy) (Image)
This medication is also very cardiotoxic, so an echocardiogram is required before starting therapy.
Cyclophosphamide
This is typically given with doxorubicin in a combination known as “AC” (not followed by DC), but we may also give it with docetaxel (TC). It also works to damage cell DNA.
Side effects include low blood counts, mouth sores, and bladder irritation.
Sacituzumab govitecan (Trodelvy)
This is another antibody-drug conjugate. It is made of an antibody that targets Trop-2 (a protein highly expressed on many breast cancer cells) linked to a chemotherapy drug.
Side effects include low white blood cells, diarrhea, and hair loss.
Pembrolizumab
This is our splash of immunotherapy in the breast cancer world! (Image) It works by helping the immune system attack cancer cells.
Normally, cancer cells can “turn off” immune cells by using a pathway called PD-1/PD-L1. Pembrolizumab blocks PD-1 on immune cells, which turns the immune response back on so the body can recognize and destroy the cancer. We typically use this in TNBC.
Side effects include skin reactions, diarrhea, fatigue, and muscle/joint pain.
There is your crash course on chemotherapy used in breast cancer! So how do we use these agents? We use these in different combinations depending on the “what/where” of the cancer.
I know! This is a LOT of information! And this is still tl;dr (and we’re getting close to the dr portion). So, to bring this all into a more digestible diagram – you know what we have to do!
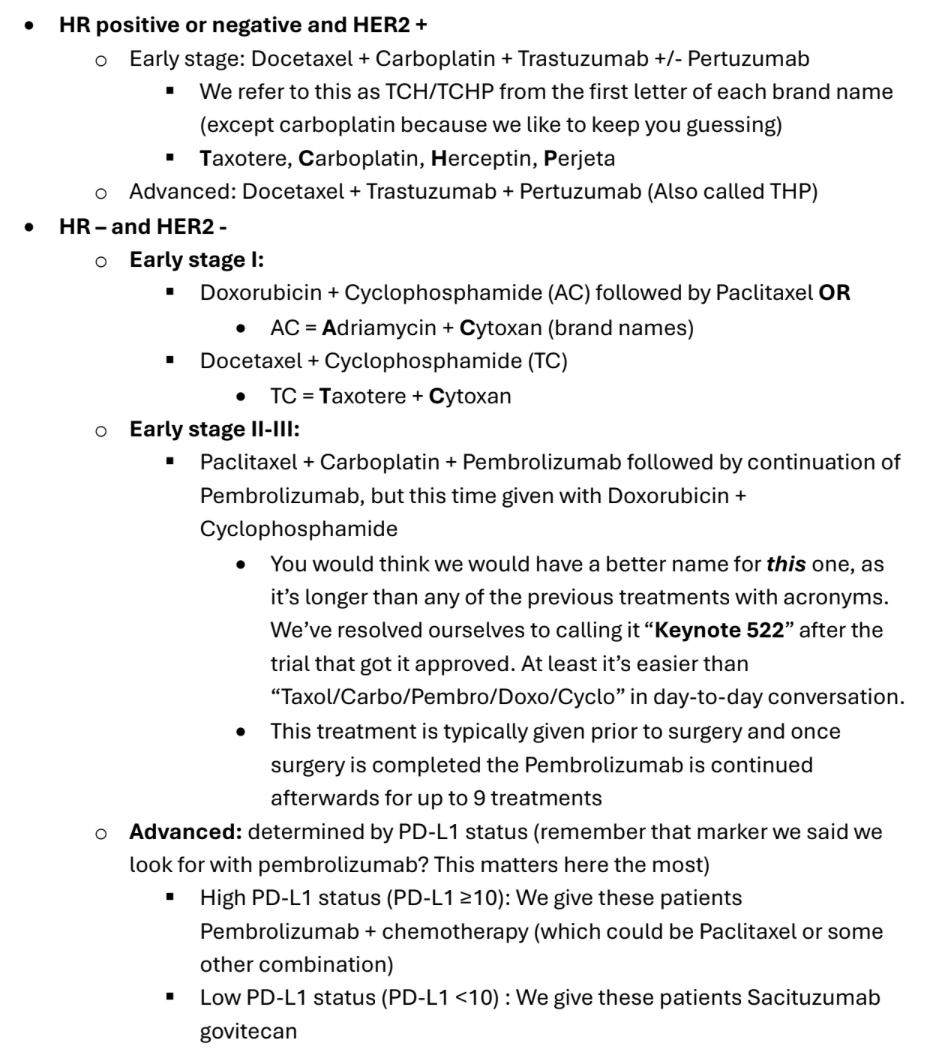
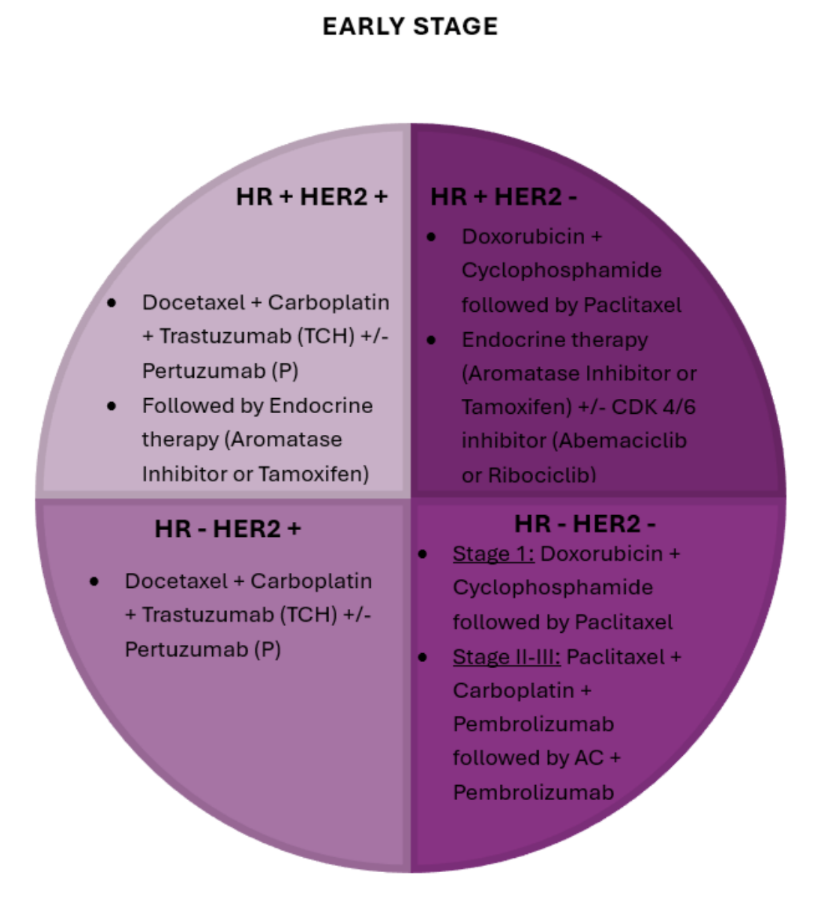
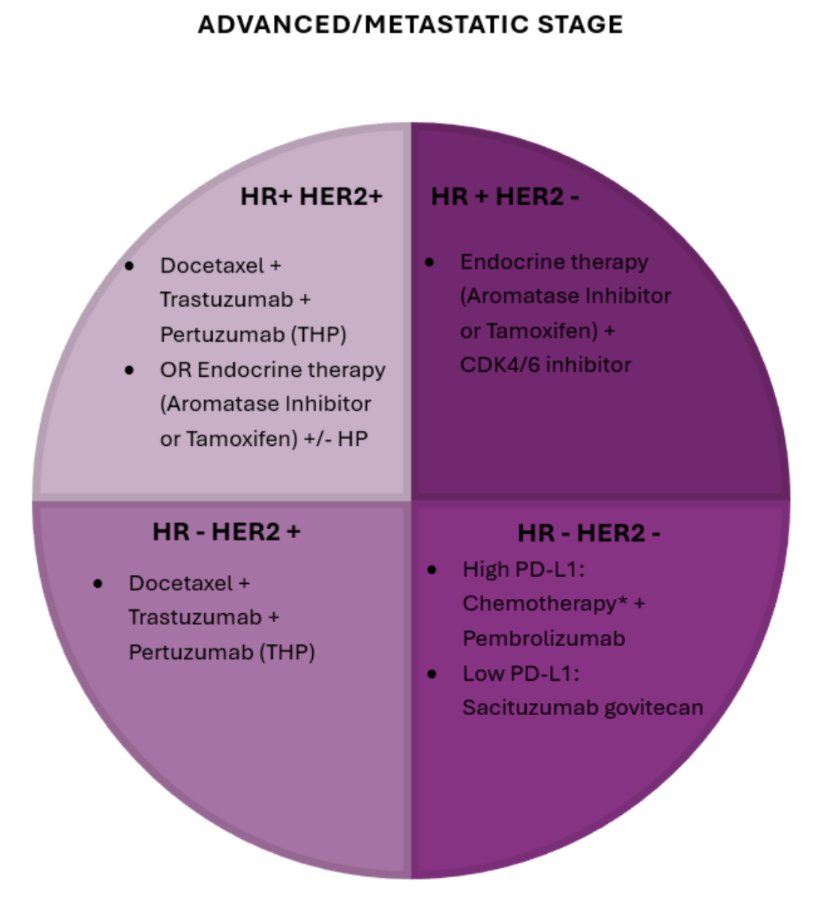
Now get ready for the BCTSG! (Breast Cancer Treatment Summary Guide!)
{kind=link}
{kind=link}
*Chemotherapy could include paclitaxel or agents we have not discussed, such as albumin-bound paclitaxel or carboplatin+gemcitabine.
Of course, this doesn’t cover everything that breast cancer has to offer. If it did, there’s no way I’d be able to put it on tl;dr because it would inevitably be a dr. This barely scratches the surface of all the agents and treatments we have available, but I hope this gives you a birds-eye view of the most common/standard treatments you may see!
Breast cancer treatment is changing so rapidly! Even during the making of this article, more things are switching to first line, and new combinations are being approved. But that’s one of the exciting things about being a pharmacist, right? There’s always more to learn!