
The tl;dr Case of the Month: HIV
A note from the tl;dr team: As you are already aware, the practice of pharmacy is constantly evolving. Our profession is shifting from medication dispensing toward a more clinically focused role centered on pharmacotherapy management.

Nicholas knows… Change is a breath of fresh air!
Gone are the days of calculating mEq at work. Instead, we are expected to understand pharmacodynamics, pharmacokinetics, guideline directed therapy, and key clinical pearls.
Here at tl;dr pharmacy, we welcome these changes. (Image) So much so that we are testing out a brand new case of the month series. These cases are meant to provide practical, real-world learning opportunities to help you prepare for rotations, the NAPLEX, board exams, and your future career.
The format is simple:
You’ll receive a patient case (found below)
Followed by several multiple-choice questions
If you keep on reading, you will see a review of the correct answers with short bullet point key takeaways
With all that being said, let’s dive in.
P.S. If there is a specific topic that you would like us to cover in a future case, feel free to reach out to me at josef@tldrpharmacy.com.
Meet Your Patient
Patient: RT
Age: 32 years
Sex: Male
Weight: 77.9 kg
Vitals: BP (118/76 mmHg), HR (96 bpm), RR (17 breaths/min), Temp (98.3 ℉), O2 Saturation (96%)
Subjective
RT is a 32-year-old male who presents to your HIV clinic for medication refill requests. He admits to poor adherence over the past several months but is motivated to “get his life back together.” He is unsure of what medications he is supposed to be taking and admits to poor adherence to his lab draws.
Objective
Past Medical History: HIV, IV Drug Misuse, Hypertension
Home Medications: unknown at this time
Assessment
CBC: pending
CMP: pending
HIV Viral Load: 141,000 copies/mL (normal: undetectable)
CD4 Count: 87 cells/uL (normal: 500-1500 cell/uL)
Imaging (Chest X-Ray): no evidence of developing segmental infiltrates or pleural effusions
Time for the questions…
1) Antimicrobial prophylaxis should be started for which of the following opportunistic infections? (select all that apply)
a) Pneumocystis Jiroveci Pneumonia
b) Cytomegalovirus
c) Mycobacterium Avium Complex
d) Toxoplasmosis
e) Treponema pallidum
2) Which prophylactic antimicrobial should be started for this patient?
a) Azithromycin
b) Voriconazole
c) Sulfamethoxazole/Trimethoprim
d) Amphotericin B
e) Cefepime
3) How long should antimicrobial prophylaxis be continued for this patient?
a) Once CD4 count exceeds 100 cells/uL for 3 consecutive months
b) Once CD4 count exceeds 100 cells/uL for 6 consecutive months
c) Once CD4 count exceeds 200 cells/uL for 3 consecutive months
d) Once CD4 count exceeds 200 cells/uL for 6 consecutive months
e) Once CD4 count exceeds 200 cells/uL for 12 consecutive months
4) Which of the following antiretroviral regimen(s) is/are recommended to start for this patient? (select all that apply)
a) Bictegravir/emtricitabine/tenofovir alafenamide
b) Dolutegravir/abacavir/lamivudine
c) Abacavir/darunavir/atazanavir
d) Lamivudine/ritonavir/cobicistat
e) Enfuvirtide/maraviroc/cobicistat
5) Which of the following best describes the drug class and mechanism of action of dolutegravir?
a) Integrase Strand Transfer Inhibitor (INSTI); binds to the integrase active site and inhibits the strand transfer step of HIV-1 DNA integration necessary for the HIV replication cycle
b) Nucleoside Reverse Transcriptase Inhibitor (NRTI); binds to reverse transcriptase and blocks the RNA-dependent and DNA-dependent DNA polymerase activities
c) Non-Nucleoside Reverse Transcriptase Inhibitor (NNRTI); interferes with HIV viral RNA-dependent and DNA-dependent DNA polymerase resulting in inhibition of viral replication
d) Fusion Inhibitor; binds to the gp41 subunit and inhibits the fusion of HIV-1 virus with CD4 cells by blocking the conformational change in gp41 required for membrane fusion and entry into CD4 cells
e) Protease Inhibitors (PI); binds to the site of HIV-1 protease activity and inhibits cleavage of viral polyprotein precursors into individual functional proteins required for infectious HIV
6) Which best describes the seven stages of the HIV life cycle?
a) Fusion → Integration → Replication → Assembly → Binding → Reverse Transcription → Budding & Maturation
b) Integration → Reverse Transcription → Fusion → Budding & Maturation → Assembly → Binding → Replication
c) Budding & Maturation → Fusion → Assembly → Integration → Reverse Transcription → Binding → Replication
d) Binding → Reverse Transcription → Integration → Replication → Assembly → Budding & Maturation → Fusion
e) Binding → Fusion → Reverse Transcription → Integration → Replication → Assembly → Budding & Maturation
Okay ready for the answers? Don’t cheat and look down here first!
Answers:
1) A & D
2) C
3) C
4) A & B
5) A
6) E
Need more HIV NAPLEX review?
Just a heads up here. This is NOT going to be an all inclusive guide to HIV. There is a lot more to HIV that you may need to know. So if you’re looking for a full review, this is not the place. Good news though. Here at tl;dr we generally have all of our bases covered. So if you want a full in-depth review, take a peek below :)
HIV Bootcamp Series can be found here, here, here, here, here, here, and here
What Every Pharmacist Should Know about HIV Pre-Exposure Prophylaxis (PrEP)
What Every Pharmacist Should Know about HIV Post-Exposure Prophylaxis (PEP)
I know, Dwight - I think our repository of HIV posts is rather impressive too!
I wasn’t lying. We’ve literally written about every HIV topic that you will need to know for the NAPLEX. Anything to make your lives easier :). And if all that still isn’t enough, then check out our NAPLEX practice exam and private NAPLEX tutoring. (Image)
Okay I digress. Let’s get into the case now.
Time for Topic Review
There are 3 main HIV topics that you’ll likely get tested on. So please put them to memory. These topics include:
HIV replication cycle and which step each antiretroviral class inhibits
Opportunistic infections & treatment (specifically, PJP, toxoplasmosis, and MAC)
HIV treatment backbone & clinical pearls of the common HIV meds
Questions 1-3: Opportunistic Infections
Very very quick review time: HIV infects and destroys CD4 lymphocytes. CD4 lymphocytes are key in helping provide immune protection. Without CD4, you become immunocompromised and prone to infections to pathogens that your body normally fights off.
Those are called opportunistic infections.
There are 3 opportunistic infections that you should know for the NAPLEX: Pneumocystis Jiroveci Pneumonia (PJP), toxoplasmosis, and Mycobacterium Avium Complex (MAC). The CD4 count is your best friend to help you determine when you need to cover for what. Once you have those memorized, the rest is easy.
CD4 <200 cells/uL:
Cover for: PJP
Treatment of choice: Bactrim
When to stop prophylactic therapy: CD4 ≥200 for ≥3 months on antiretroviral and viral load suppressed
CD4 <100 cells/uL:
Cover for: Toxoplasmosis
Treatment of choice: Bactrim
When to stop prophylactic therapy: CD4 ≥200 for ≥3 months on antiretroviral and viral load suppressed
CD4 <50 cells/uL:
Cover for: MAC
Treatment of choice: Azithromycin
When to stop prophylactic therapy: No symptoms of MAC AND CD4 ≥100 for ≥6 months
Now that we have that info, let’s review our case. Our patient has uncontrolled HIV secondary to poor medication adherence as evident by his low CD4 count and high HIV viral load. This puts him at risk for opportunistic infections.
Step 1 is to look at the CD4 count, which resulted at 87 cells/uL. Per our algorithm above, his CD4 count is <100 cells/uL, making him at risk for both PJP and toxoplasmosis (answer to question 1). Luckily, Bactrim covers both of those infections, thus making it the treatment of choice (answer to question 2). And in regard to how long you continue prophylactic Bactrim, it’s until the patient is adherent to his HIV meds and the CD4 recovers to ≥200 for ≥3 months and viral load is suppressed (answer to question 3).
Pretty straightforward, right?
Questions 4-6: HIV Replication Cycle, Treatment, and MOA
To better understand how antiretrovirals work, I think it’s important we first review the HIV replication cycle. There are a total of 7 steps in HIV replication: Binding → Fusion → Reverse Transcription → Integration → Replication → Assembly → Budding & Maturation (answer to question 6). HIV meds inhibit one (or more) of those steps and prevent the replication of HIV, leading to viral load suppression.
There are six main antiretroviral (ART) drug classes used to treat HIV:
1. Nucleoside Reverse Transcriptase Inhibitors (NRTIs):
MOA: block viral reverse transcriptase by chain termination
Common agents: Typically end in “-ine” (with some exceptions)
Examples: Abacavir (need to screen for HLA-B*5701 for hypersensitivity reactions), Lamivudine, Emtricitabine, Tenofovir disoproxil (more renal toxicity), Tenofovir alafedanamide, Zidovudine
2. Non-Nucleoside Reverse Transcriptase Inhibitors (NNRTIs):
MOA: directly inhibit reverse transcriptase enzyme
Common agents:
Examples: Efavirenz (psychiatric conditions), Rilpivirine (can’t be used with PPIs)
3. Integrase Strand Transfer Inhibitors (INSTIs):
MOA: prevent integration of viral DNA into host genome
Common Agents: Typically end in “-gravir”
Examples: elvitegravir, bictegravir, dolutegravir, raltegravir
4. Protease Inhibitors (PIs):
MOA: Prevent maturation of new virions
Common Agents: Typically end in “-navir”
Examples: Darunavir, Atazanavir, Fosamprenavir
Clinical Pearl: commonly used with cobicistat as a booster. Cobicistat has no direct activity on HIV. It acts as a pharmacokinetic enhancer (booster) by acting as a potent inhibitor of CYP3A4, leading to increased plasma concentrations of PIs
5. Entry Inhibitors (CCR5 Antagonist):
MOA: block viral attachment/entry into CD4 cells
Common Agents: maraviroc, ibalizumab
6. Fusion Inhibitors:
MOA: prevent fusion of HIV envelope with host membrane
Example: enfuvirtide
For you visual learners, take a look at the picture below. It perfectly explains the HIV replication cycle and even shows you which step each HIV antiretroviral inhibits. (Image)
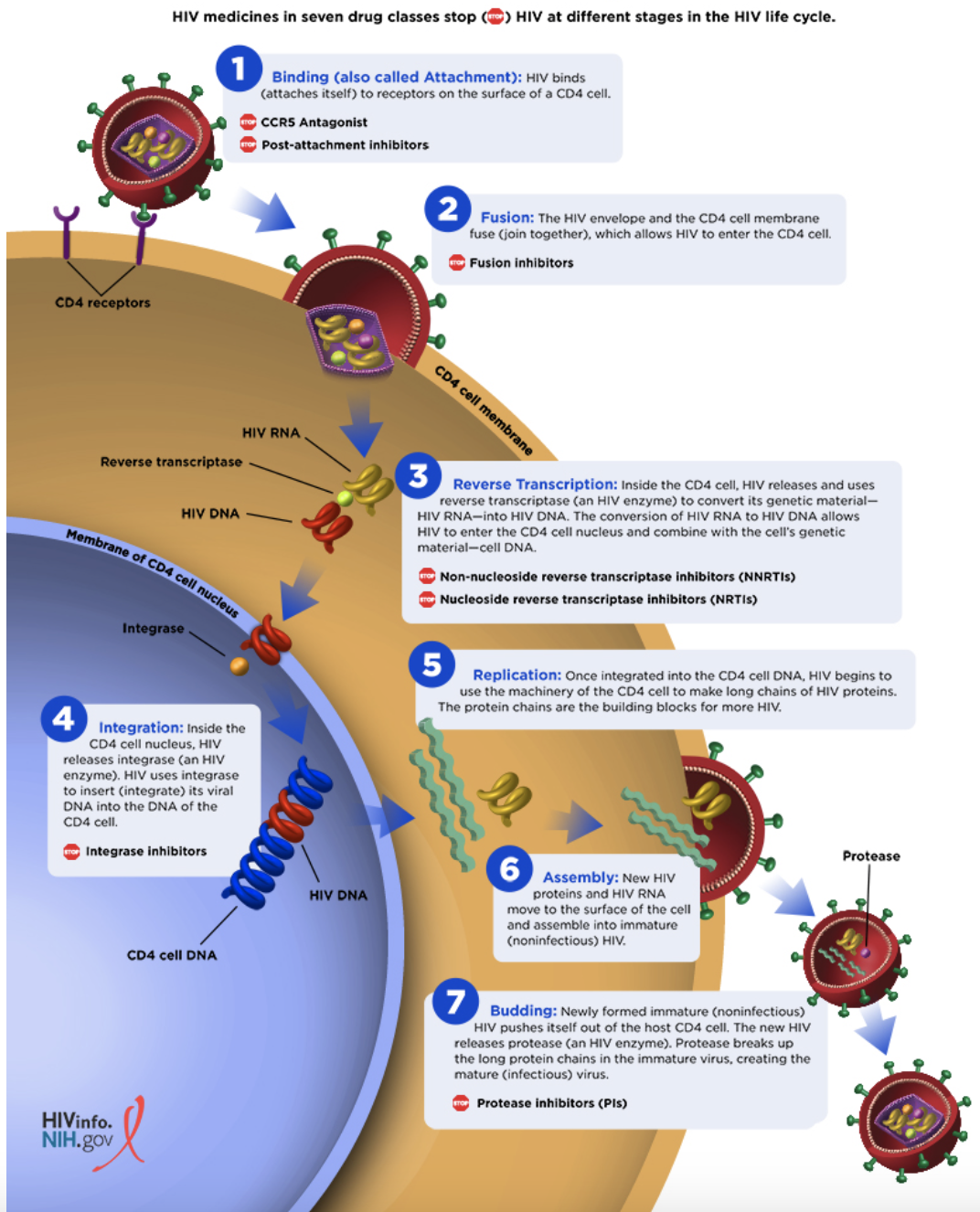
Okay now back to our case to answer question 5. Dolutegravir ends in “-gravir”. Therefore it must belong to the INSTI class. And we now know that INSTIs work by preventing the integration of viral DNA into the host genome.
That leaves us with just one more question. This is the final main point that you’re going to have to remember. The HIV treatment backbone is 2 NRTIs + 1 INSTI.
Anytime you’re asked to come up with a regimen to treat HIV, your answer should always have a total of 3 agents that include two NRTIs and one INSTI. So, looking at the fourth question, only the top two regimens have 2 NRTIs and 1 INSTI. The other options don’t have that recommended backbone and are therefore incorrect.
Alright, that’s all folks! I hope you found this helpful and good practice! Again, if you have any recommended case of the month topics, please don’t hesitate to reach out to us!