
What Every Pharmacist Should Know about Breast Cancer: Part 1
Steph’s Note: This week, we’re dipping our toes into a therapeutic corner we haven’t dared touch in a while…oncology. *cue big booms of thunder and cracking lightning* All jokes aside, I’m glad we have Clarissa here to demystify this topic for us.
Clarissa Wilkins, PharmD, BCOP is an Oncology Pharmacist in the Treatment Review and Coordination Team at Texas Oncology. She graduated from the University of the Incarnate Word pharmacy school in 2017 (despite her worst class being – ironically – Oncology) and started out as a pediatric pharmacist while gradually descending into madness as oncology continued to haunt her until she finally threw in the towel and has now been a dedicated oncology pharmacist for 7 years. Outside of work she’s a video game-aholic and an avid fantasy/sci-fi reader.
Oncology – at least for me – was the part of pharmacy school journey where I thought, “Do I actually want to be a pharmacist?” I quickly lied told myself that it was only one class, and I would never need to see it again. Nine years later here I am, a board-certified oncology pharmacist.
How did I let this happen? (Image)

Well, once you peel back the scary, hazardous, exterior layers, however many of them there may be, you find out oncology isn’t so different from every other disease state. Sure, we like to use long unpronounceable names (looking at you talimogenelaherparepvec)…and we may add 4 nonsensical letters to the end of every monoclonal antibody…and we may also need to wear a spacesuit to touch them…
Wait a second, where did I put that “but”…?
BUT (ah HA, there it is!), once you break it down, it’s not the big scary beast we make it out to be! It can be an extremely rewarding field of practice.
Luckily for you, a big starting point for all things oncology is already available here at tl;dr. Not only is there a 7300-word oncology overview (that even ends on an 80s pop song reference), but there’s also a post on chemotherapy induced nausea and vomiting (CINV) and supportive care, which are HUGE in the oncology world. I suggest you check out the awesome resources tl;dr has to offer. Since you’ve already had an introduction, I’m going to be taking you straight into my favorite area of oncology: breast cancer.
Even if you’re not in an oncology area, I’m sure you’ve had your fair share of breast cancer exposure - whether it’s on your social media account in October, a pink ribbon here and there, or those bracelets back in the 2000s that said "i ♥ boobies!" that your school tried to ban. (Image)
Unfortunately, despite my teenage-self arguing that that bracelet would cure cancer to the principal, it’s still a top player in the world of oncology.
One in 8 women in the United States will be diagnosed with breast cancer in their lifetime. While advances in screening and testing have reduced the overall risk of death, the number of people diagnosed continues to rise. In 2025, it was estimated that 316,950 women and 2,800 men would be diagnosed with invasive breast cancer, and that’s in addition to the estimated 59,080 new cases of non-invasive breast cancer (we will get to those differences in a second). An estimated 42,170 women died from breast cancer in 2025.
However, it’s not all doom and gloom. When it’s caught early, the 5-year relative survival rate is 99%! This is why advances in screening and testing are so important! There are several things that factor into breast cancer, so let’s start with risks: (Image)
Sex: of course, being a woman, or a person assigned female at birth, is the most important risk factor.
Age: just like other diseases, your risk of breast cancer increases the older you get. Two out of three invasive breast cancers are found in women 55 and older.
Family History/Genetics: if you have family members who have been diagnosed with breast cancer, there is a higher risk of developing the disease yourself.
Race: although Caucasian women are slightly more likely to develop breast cancer, African American women are more likely to develop more aggressive, more advanced-stage breast cancer diagnosed at a young age.
Pregnancy History: the age a woman has her first child and the number of times a woman has given birth can affect your risk of developing breast cancer.
Side note: breastfeeding can actually lower the risk of breast cancer, especially if you breastfeed for longer than one year.
Menstrual History: women who have their first period prior to turning 12 years of age have a higher risk of breast cancer later in life.
Hormone Therapy: this can be replacement therapy or birth control. Both may increase your risk of breast cancer.
Dense Breast Tissue: can make finding lumps harder to detect.
Radiation Therapy: any radiation to the chest prior to 30 years of age.
And, of course, you have the classic modifiable risk factors including lack of exercise, obesity, smoking, and alcohol.
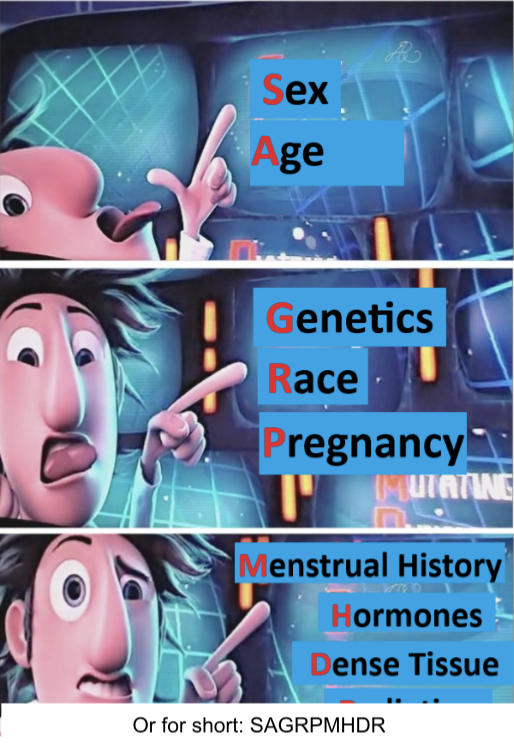
Flint Lockwood’s got the breast cancer risk factors down pat. Do you?
Now, all that being said, 60-70% of people with breast cancer have no connection to these risk factors, and some people with these risk factors never develop cancer. Cancer likes to keep us guessing.
We’ve thrown around a couple words like invasive and non-invasive. There are several different types of breast cancer, and these are generally decided by a couple of things:
The location in the breast where the tumor is growing,
How much the cancer has grown, and
Certain features that influence how the cancer behaves.
I’m going to lump the first two bullets together and call them Question #1.
Question #1: Where is the Cancer?
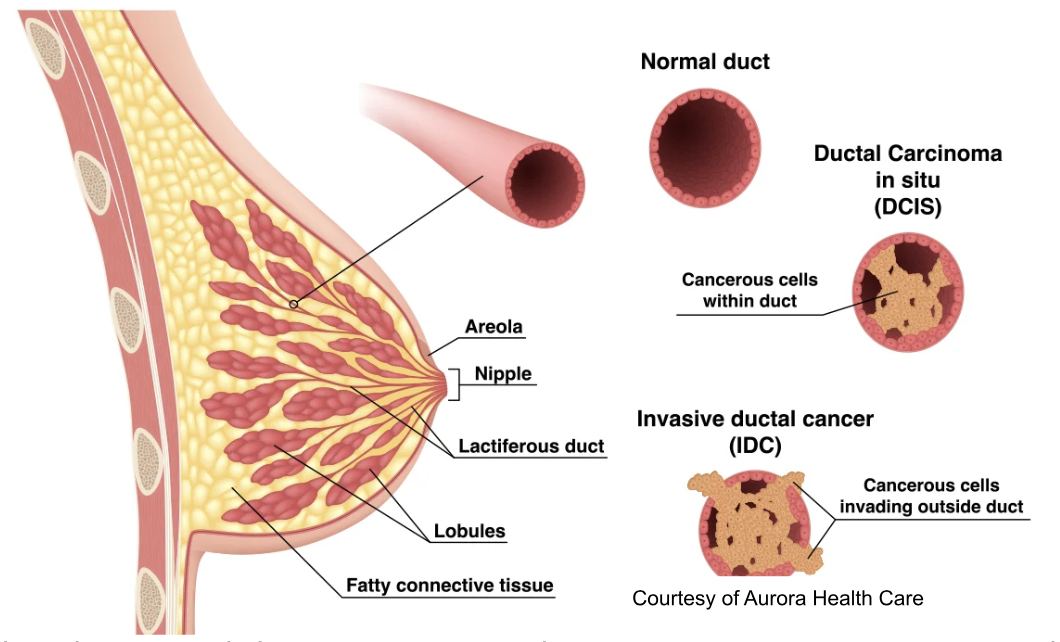
Non-invasive breast cancer is breast cancer that has not spread beyond the breast tissue where it originated from. There are two types: Ductal carcinoma in situ (DCIS), which means it has not spread outside the milk ducts where it started, and Lobular carcinoma in situ (LCIS), which means it has not spread outside the lobules where it started. These are generally deemed pre-cancerous and are typically treated with a lumpectomy, where the cancerous tissue and surrounding tissue is removed. Surgery is followed by radiation to keep it from coming back, and sometimes there are also medications, which we will go through later!
Invasive breast cancer is the more aggressive cancer that has spread into the surrounding breast tissue. And just like with non-invasive, we have Invasive ductal carcinoma (IDC) – you guessed it, it starts in the milk ducts - and Invasive lobular carcinoma (ILC) – guessed it again, starts in the lobules. (Image)
Then there is metastatic breast cancer, meaning that it has spread to other organs in the body. Typically, breast cancer spreads to the bones, lungs, liver, or brain.
All of these help determine what stage of breast cancer the patient has:
Stage 0: Non-invasive, and has not spread
Stage 1: Invasive, has spread to the surrounding normal tissue/lymph nodes
Stage 2: Invasive, has spread but it is still contained in the breast tissue or growth has only extended to axillary lymph node
Stage 3: Invasive, has spread out of the immediate, or local, area in the breast and into the lymph nodes or muscles close to the breast. What we call “Locally Advanced” breast cancer.
Stage 4: Advanced breast cancer that has spread to other organs
Now I could go on and on about all the different types of breast cancer, but this is tl;dr, so we are going to focus on the ones that help determine how we treat a patient with systemic therapy. Now that we’ve discussed how ‘where’ the cancer is helps guide how we treat it, let’s get into the ‘what’.
Question #2: What is the cancer?
The characteristics of cancer cells are some of the most important aspects of deciding how we are going to treat it. The main ones we are going to talk about are hormone receptor status and HER2 status.
Hormone Receptor Status

{kind=link}
Breast cancer can have an estrogen receptor (ER) status and a progesterone receptor (PR) status. If the cancer cell is ER-positive (ER+), this means that the cancer cell uses estrogen to grow and multiply. (Image) The higher the percentage of ER+ cells, the better the prognosis (because we have great medications to deal with this!). The same goes for PR-positive (PR+), except this is when the cancer uses progesterone. Breast cancer can be both ER/PR+, or it can be just one. Either way, we will treat these cancers with some form of hormonal therapy.
{kind=link}
HER2 Receptor Status
Human epidermal growth factor receptor 2, or simply HER2, is a type of receptor that can be found on the surface of breast cancer cells. HER2-positive breast cancers tend to be faster growing, more aggressive, and are diagnosed at a later stage. Breast cancer can be HER2-negative, HER2-low, or HER2-positive. However, like with the ER/PR+ breast cancers, we have specific medications that can target HER2 receptors.
But Clarissa, what if the cancer has NONE of these? What do we do?
We call this Triple Negative Breast Cancer (TNBC). It’s more commonly found in younger women, African American women, or in people with a BRCA1 mutation – a genetic mutation that can lead to various aggressive cancers. In this situation, the cancer lacks estrogen, progesterone, and HER2 targets, which means we can’t use any of our targeted tactics to kill it. In these cancers, we can only stick with our classic chemotherapy agents, as well as immunotherapy.
So that’s your tl;dr introduction to the world of breast cancer! Let’s wrap it all up!
Breast cancer is still a major player in oncology to this day.
Where the cancer is located makes a difference in treatment.
Non-Invasive vs Invasive
Ductal vs Lobular
Characteristics of the tumor help us determine treatment.
Hormone receptor status
HER2 status
I know you’re all thinking, “But Clarissa – you’ve told us these things help determine treatment, so what are the treatments?” Have no fear, my friends! In our next article, we will be breaking down the treatment options, so stay tuned!