
The tl;dr Case of the Month: Atrial Fibrillation
A note from the tl;dr team: in case you didn’t already know, we recently launched our new case of the month series. So far, we’ve gone live with our HIV and community-acquired pneumonia cases. If you haven't already done so, feel free to check them out and test your knowledge :).
Since we’ve only focused on infectious diseases so far, I figured it’d be nice if we switch things up and attack a different organ. And what better organ than the heart.
So folks, strap in and let’s conquer this case together. And remember, if you get an answer wrong, keep scrolling down, and you’ll see the rationale for each question and why every answer is correct or incorrect.
P.S. If there is a specific topic that you would like us to cover in a future case, feel free to reach out to me at josef@tldrpharmacy.com.
Meet Your Patient
Patient: PY
Age: 56 years
Sex: Male
Weight: 79.3 kg
Vitals: BP (148/90 mmHg), HR (138 bpm), RR (14 breaths/min), Temp (98.1 °F), O2 Saturation (97%)
Subjective: PY presents to your clinic from home c/o palpitations, fatigue, chest discomfort, and dizziness. He claims that symptoms have persisted for a few weeks and do not go away at rest.
Objective
Past Medical History: HTN, T2DM, MI s/p drug-eluting stent circa 2018, HFrEF, BPH, CKD Stage II
Home Medications: Losartan 50 mg QD, Aspirin 81 mg QD, Atorvastatin 40 mg QD, Metformin 500 mg BID, Sitagliptin 100 mg QD, Finasteride 5 mg QD, Tamsulosin 0.4 mg QD, Spironolactone 50 mg QD
Allergies: Bees (anaphylaxis); NKDA
Assessment
CBC: All labs WNL
CMP: Creatinine (1.35 mg/dL); all other levels WNL
Imaging (Chest X-Ray): within normal limits
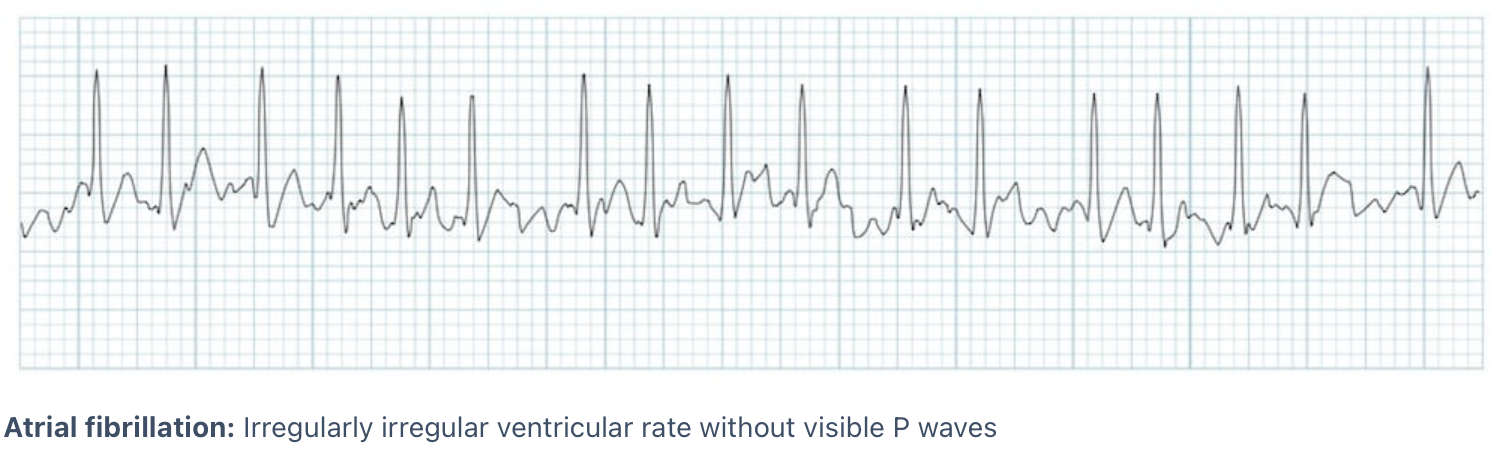
EKG: Atrial fibrillation with rapid ventricular response (Image)
The attending physician is concerned for new-onset atrial fibrillation and would like to start therapy. Which of the following medications is most appropriate to start at this time?
a) Diltiazem
b) Bisoprolol
c) Amiodarone
d) Flecainide
e) Patient should undergo electrical cardioversion
According to the 2023 ACC/AHA/ACCP/HRS Guideline for the Management of Atrial Fibrillation, what is the recommended target resting heart rate for patients with atrial fibrillation and HFrEF undergoing a rate-control strategy?
a) <60 bpm
b) <80 bpm
c) <100 bpm
d) <110 bpm
e) <120 bpm
Which of the following correctly identifies this patient’s CHADS-VASc score and the most appropriate stroke prevention strategy?
a) 1; no anticoagulation indicated
b) 2; anticoagulation should be considered
c) 4; anticoagulation should be started
d) 5; anticoagulation and antiplatelet therapy should be started
e) 6; fibrinolytic therapy should be considered
The attending provider would like to initiate apixaban. Which regimen is most appropriate to start?
a) Apixaban 10 mg PO BID, followed by 5 mg BID thereafter
b) Apixaban 15 mg PO BID, followed by 20 mg once daily thereafter
c) Apixaban 2.5 mg PO BID
d) Apixaban 5mg PO BID
e) Apixaban 10 mg PO BID
According to the American College of Chest Physicians (CHEST), patients with atrial fibrillation lasting >48 hours should receive at least ___ weeks of therapeutic anticoagulation before cardioversion and at least ___ weeks after cardioversion.
a) 2,2
b) 2,3
c) 3,4
d) 4,5
e) 6,6
Several months have passed and the provider would like to initiate amiodarone for rhythm control. Which of the following drug-drug interactions should be monitored if amiodarone is initiated?
a) Amiodarone & Atorvastatin
b) Amiodarone & Finasteride
c) Amiodarone & Metformin
d) Amiodarone & Sitagliptin
e) Amiodarone & Aspirin
Okay ready for the answers? Take a look below:
1) B
2) B
3) C
4) D
5) C
6) A
Need More Atrial Fibrillation NAPLEX Review?
Just a heads up here. This is NOT going to be an all inclusive guide to atrial fibrillation. It will definitely test you on the important topics of afib, but it’s not going to include every teeny tiny detail. But I have good news! Here at tl;dr, we like to have our bases covered. If you do want a full crash course on atrial fibrillation, then check out our article, which can be found here. And in case you want a little more, check out our pocket guides, which can be convenient to have on rounds.
And if all that still isn’t enough, then feel free to sign up for our private 1-on-1 NAPLEX tutoring, and we will cover everything cardiovascular. Lastly, if you want more questions like this, then check out our NAPLEX practice exam.
Okay I digress. Let’s dive into the case now.
Review Time
I can guarantee that you will get some form of atrial fibrillation question on your next board exam. Typically, the topics you should familiarize yourself with include:
Calculating CHADS-VASc score
Knowing how to interpret CHADS-VASc score
Rate vs rhythm control
Anticoagulation of choice and dosing
Antiarrhythmic drug interactions and toxicities
With that being said, let’s see how our case incorporates all these topics :).
Questions 3 & 4: Calculating and Interpreting the CHADS-VASc Score
There’s no dodging this. If you see afib, you will see CHADS-VASc. You’re going to have to memorize how to calculate it and what the heck the score even means. So let’s review.
Remember learning about the left atrial appendage in the heart? You know that tiny little pocket in the left atrium that does absolutely nothing for us? Here’s a pic in case you need a refresher (Image):
Well, if you have atrial fibrillation, your left atrium isn’t pumping effectively. And as a result, blood doesn’t get pushed out as well and begins to pool in that left appendage. And if blood pools for too long, it can clot. Eventually, that clot can displace from the left appendage, and the heart will pump it out of the atrium and into your brain, causing a stroke. To prevent this, we start blood thinners for high-risk afib patients.
Important point here - the blood thinner does NOT treat atrial fibrillation. It’s primarily used for prevention of stroke in patients with atrial fibrillation. So, how do we determine who is high risk and needs a blood thinner? The CHADS-VASc score, of course!
Calculating CHADS-VASc is pretty straight forward. Take a peek below:
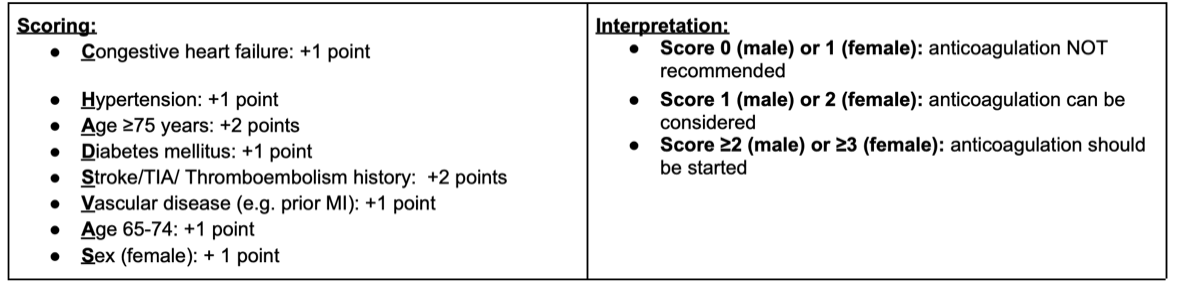
Notice on the interpretation that being female in and of itself isn’t enough of a reason to start anticoagulation. So if the only point on the scale is from sex/being female, that doesn’t automatically buy anticoagulation. Females have to have at least 1 other risk factor to consider anticoagulation.
Now that we have this info, let’s apply it to our patient case to help us answer questions 3 and 4. To calculate this patient’s CHADS-VASc, he gets the following points:
CHF (+1 point), Hypertension (+1 point), Diabetes (+1 point), Vascular Disease (+1 point).
That gives us a total of 4 points which gives us our answer to question 3. The next step is to interpret our score. Based on the table above, any male with a CHADS-VASc score ≥2 should be started on anticoagulation since their 10-year risk of a stroke is higher than their risk for bleeding. When it comes to medicine, it’s always about risk vs benefit. And given this patient’s high score of 4, anticoagulation should be started.
Great. So we know that we need to start a blood thinner. But which one? The American College of Cardiology recommends DOACs as first-line therapy over warfarin for stroke prevention in patients with atrial fibrillation who do NOT have rheumatic mitral stenosis or a mechanical heart valve. You have 4 options to pick from the DOAC class, and these include apixaban, rivaroxaban, edoxaban, and dabigatran.
If your patient has afib and mechanical heart valves or moderate-to-severe rheumatic mitral stenosis, then warfarin is the anticoagulant of choice. All that being said, when it comes to practical use, probably 90% of atrial fibrillation patients will be started on either apixaban or rivaroxaban.
Surprise surprise, the physician wants to start apixaban. The next step is knowing the dose. You will have to know the doses of all the DOACs for all the different indications. For starters, remember that patients with atrial fibrillation do NOT need to be loaded. Loading is only necessary when you’re treating an acute clot such as a VTE. Remember, anticoagulation here is preventative. We’re not necessarily treating an acute clot like we are in VTE. We are preventing the clot from forming to prevent a stroke.
Regarding apixaban dosing, remember these clinical pearls:
A load is not necessary when treating atrial fibrillation
General dosing for atrial fibrillation is 5 mg PO BID
Dose adjustment to 2.5 mg PO BID is only needed if your patient has 2 or more of the 3 criteria:
Age ≥80 years old,
Body Weight ≤60 kg, or
Scr ≥1.5 mg/dL
Looking at our patient, he is not greater than 80 years old, weighs more than 60 kg, and has a Scr less than 1.5 md/dL. Therefore, he does NOT meet dose reduction criteria, and 5 mg PO BID should be started (question 4).
Questions 1, 2, 5, & 6 : Rate Control vs Rhythm Control vs Electrical Cardioversion
This has been a topic of debate for years. When it comes to the acute treatment of atrial fibrillation, you have 3 major treatment pathways:
Rate control
Definition: control the rate without attempting to restore normal sinus rhythm (patient remains in afib)
Place in Therapy: generally first-line for most patients with persistent/permanent afib, especially in older and asymptomatic patients
Common agents: beta-blockers, non-DHP calcium channel blockers, digoxin
Rhythm control (aka chemical/pharmacological cardioversion):
Definition: restore and maintain sinus rhythm
Place in Therapy: generally second-line for patients who are symptomatic despite adequate rate control
Common agents: amiodarone, flecainide, propafenone, dofetilide
Electric cardioversion (aka ride the lightning):
Definition: deliver a synchronized electrical shock to restore normal sinus rhythm
Place in Therapy: hemodynamically unstable atrial fibrillation patients (e.g., hypotensive, shock, ischemic chest pain, pulmonary edema)
Let’s dive into the shallow end. I’m not going to get into the super specifics of rate vs rhythm control here. We’re only going to talk about the big picture.
Numerous studies have been published over the years to compare rate vs rhythm control for the treatment of atrial fibrillation. Long story short, these studies generally conclude comparable clinical outcomes, all-cause mortality, and cardiac morbidity and mortality. All in all, they’re pretty similar in terms of treating afib. So what’s the main difference? Safety.
Rate control agents are safer, better tolerated, have fewer drug-drug interactions, and a lot less toxicity. For example, amiodarone is a common antiarrhythmic agent used to treat afib. And if you remember, amiodarone is a potent CYP enzyme inhibitor and interacts with numerous meds (question 6). In addition, it has multiple black box warnings for pulmonary toxicity, hepatotoxicity, and cardiovascular toxicity. And if all that isn’t enough, it can prolong QTC, cause thyroid damage, and hypotension. Oh and it needs to be administered with a 0.2 micron filter because the IV form leaches plastic, which can then be infused into the patient. Yeah, it’s a pretty nasty drug lol.
So, unless you’re young, severely symptomatic, and/or have already failed a rate control agent, chances are you’re getting rate control with a beta-blocker or a non-DHP CCB.
Now let’s use this information to answer our case questions. For question 1, our patient is a younger individual who comes in with new-onset symptomatic afib. His vitals are stable, and he is not showing any signs of instability or shock. Therefore, electrical cardioversion is NOT appropriate, making answer E incorrect.
We just spent the last 10 minutes talking about why rate control is a safer initial agent for afib. So that rules out our antiarrhythmic agents, including amiodarone and flecainide (answers C & D).
We’re now left with two rate control agents: bisoprolol and diltiazem. If you read this patient’s medical history, you found that he has a history of HFrEF. This is important to know because it will help you rule out CCBs since their use is contraindicated in patients with HFrEF. In fact, beta-blockers (specifically bisoprolol, carvedilol, & metoprolol succinate) have shown mortality benefit in patients with CHF. Therefore, bisoprolol is the best option for this patient given CHF and afib. It’s a two birds with one stone typa deal.
Now moving on to question 2. We know to start rate control therapy first. But what’s our goal heart rate? Well, it depends. The 2023 ACC/AHA/ACCP/HRS Guideline for the management of atrial fibrillation recommend the following:
Patients in afib without heart failure: aim for a resting heart rate of <100 to 110 bpm
Patients in afib with HFrEF or arrhythmia-induced cardiomyopathy: aim for a resting heart rate of <80 bpm
And now onto our final question: Question 5. In the acute setting, electrical cardioversion is only indicated for hemodynamically unstable patients. However, stable patients can choose to undergo elective electric cardioversion. But there is a caveat. Patients with persistent afib who aren’t properly anticoagulated are at a higher risk for stroke since the cardioversion could restore normal sinus rhythm and displace any clot in the left appendage. To avoid all this, the American College of Chest Physicians (CHEST) recommends that patients with afib lasting >48 hours should receive at least 3 weeks of therapeutic anticoagulation before cardioversion and at least 4 weeks after cardioversion.
Well folks, that sums up our case. Hopefully you learned something new today and realized that you’re now an afib wizard. And again, if there is another topic that you want us to write a case about please shoot me an email at josef@tldpharmacy.com.