
New Drug Formulations: Loop Diuretics Part 2
Steph’s Note: This week, we’re revisiting our recent topic of new loop diuretic formulations. (If you missed part 1, check it out here.) To jog your memory, we were asking 2 critical questions while evaluating the newly approved products:
Does subcutaneous dosing produce a short-term diuretic response similar to IV furosemide?
For selected patients who present to the emergency department (ED) with worsening heart failure (HF) and can be safely discharged, can subcutaneous loop diuretics help avoid a brief admission just for IV diuresis—and potentially reduce downstream utilization and costs?
Here to shed additional light on these questions is Meredith Holmes, PharmD, BCCCP. Dr. Holmes works as a Medical Science Liaison for MannKind. Prior to that, she practiced in the Trauma ICU at an academic medical center for 12 years. Let’s see what additional new info she has for us on this topic!
P.S. Don’t forget to send your de-identified intervention stories to steph@tldrpharmacy.com for inclusion in our new Pharmacy Impact series. We want to hear the difference YOU are making and share it with the world!
When in doubt, use multiple studies, right? Very rarely - if ever - does a clinical answer come from a single study! (I mean, I guess sometimes all you have is one study…because that’s literally all that’s published on a topic. But then is that really your answer, or do you take it with a grain of salt? Mmhmm. You know. ) (Image, Image)
In this case, we’re lucky to have two more subcutaneous (SC) furosemide (FUROSCIX) studies to address the 2 questions mentioned above regarding diuretic response and hospital utilization. These studies, along with the ones discussed previously in part 1, should assist when you’re trying to understand where SC furosemide might fit.
Let’s take a look.
Study #1: Subcutaneous versus intravenous furosemide in worsening heart failure
In this 2018 randomized pilot study published in JACC Heart Failure by Gilotra et al, subcutaneous furosemide was compared to intravenous furosemide in an outpatient population with decompensated HF. Patients were randomized in an outpatient diuretic clinic to receive a single dose of furosemide, either SC or IV. It looked at total urine output over 6 hours as well as weight change, natriuresis, and adverse events.
In total, 41 patients were randomized: 19 received IV furosemide (mean dose 123 ± 47 mg) and 21 received SC furosemide (fixed dose of 80 mg over 5 hours). When the investigators looked at the main endpoint—urine output at 6 hours—the two groups were essentially the same (median IV 1,425 mL [IQR 1,075–1,950] vs median SC 1,350 mL [IQR 900–1,900]; p = 0.84). Weight loss over that same window was also similar (-1.5 ± 1.1 kg IV vs -1.5 ± 1.2 kg SC; p = 0.95).
For you visual folks, here are the results for urine output (Image):
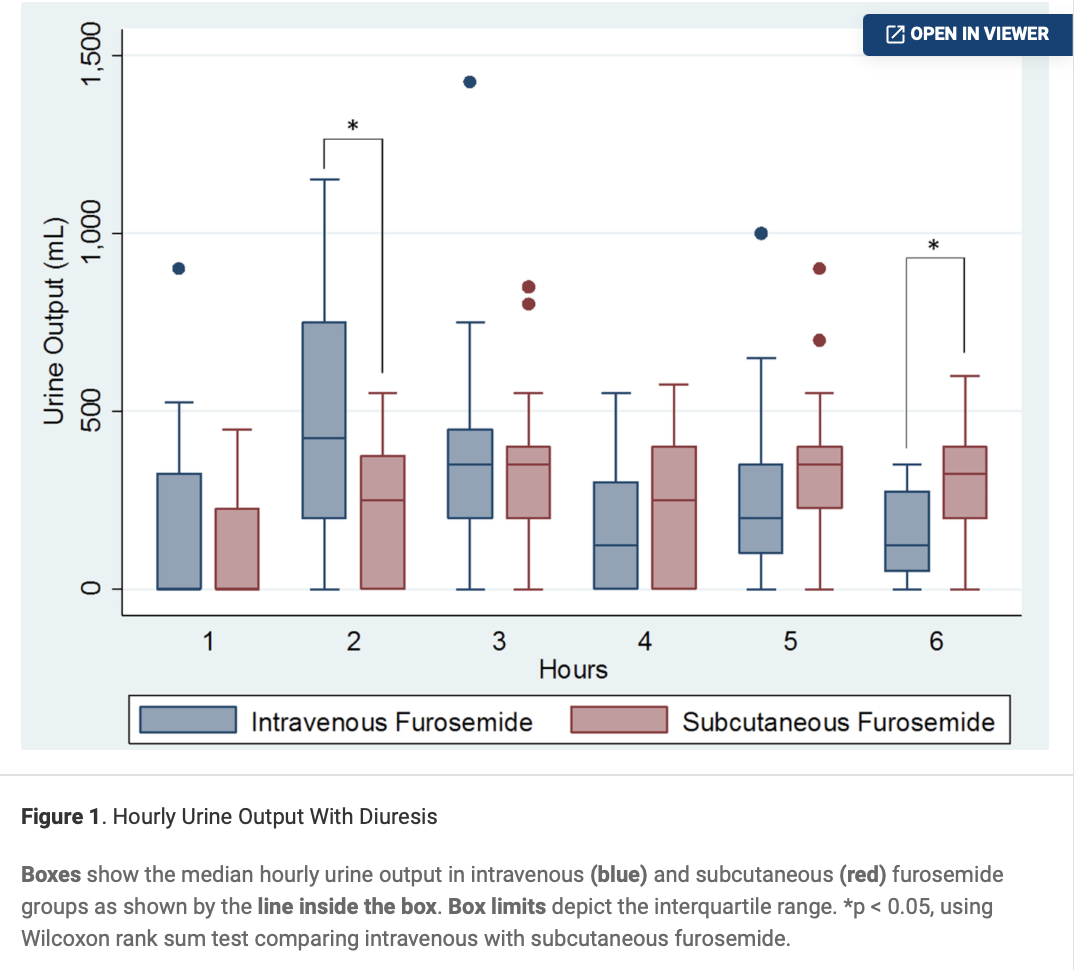
A few timing details are worth calling out. IV dosing produced more urine early on (hour 2: 425 mL IV vs 250 mL SC; p = 0.02), but by hour 6, the pattern flipped (125 mL IV vs 325 mL SC; p = 0.005). Natriuresis was higher in the SC group (7.3 ± 35.3 mEq/L IV vs 32.8 ± 43.6 mEq/L SC; p = 0.05). Safety looked similar as well. There was no worsening renal function, ototoxicity, or skin irritation with either formulation, and 30-day hospitalization rates were similar.
Now you might be asking yourselves why or how 80mg of furosemide (SC) achieved similar amounts of urine output compared with ~120 mg of IV furosemide (IV bolus)? Don’t forget the power of an infusion… The SC furosemide was given over 5 hours, whereas the IV was administered as a bolus. You can see that difference in the timing details noted above, where the IV produced earlier bigger outputs but then tapered off. The SC kept chugging along until the end, even producing significantly more urine than IV at hour 6. Sometimes the continuous application of a lower dose rather than a hot and heavy bomb works just dandy. You know…slow and steady wins the race, right?
What’s the takeaway?
Total 6-hour urine output was similar with SC furosemide versus standard IV dosing. That suggests SC delivery can achieve meaningful decongestion over a several-hour window.
On to question number 2…
Study #2: FREEDOM-HF and ED discharge with SC furosemide
The idea for the 2023 FREEDOM-HF study was simple: identify ED patients with worsening HF who were appropriate for discharge, send them home with SC furosemide (FUROSCIX, furosemide 80 mg/10 mL delivered as a 5-hour SC infusion), and then compare their outcomes with matched historical controls who were admitted for ≤ 72 hours to receive IV diuretics. Patients could receive SC furosemide up to twice per day for up to 7 doses after discharge. Exact doses were at the discretion of the physician with the goal to return patients to their maintenance oral diuretics.
The aim was to look at HF-related healthcare utilization and costs over the 30 days after ED discharge. There was a whole host of other outcomes, including rehospitalizations during follow-up, KCCQ-12, BNP/NT-proBNP, and adverse events.
The SC furosemide arm included 24 prospectively enrolled patients. Investigators identified 66 historical control patients, and the groups were well-matched for age, sex, ejection fraction (EF), renal function, and other comorbidities. Compared with these matched patients, SC furosemide patients had lower mean per-patient HF-related healthcare costs of $16,995 (p < 0.001). They also saw improvements from baseline in KCCQ-12 summary score (p = 0.0443) and BNP/NT-proBNP (p < 0.01).
Only 1 of the 24 (4.2%) SC furosemide patients was admitted to the hospital for HF during the 30 day follow up period. Compare this to the current national average of almost 25% hospital readmissions for HF within 30 days of discharge. In this study, the rate of readmission in the matched historical cohort was 7/66 (10.6%), although the difference was not statistically significant compared with the SC furosemide group.
The most common adverse events were infusion-site bruising (29%), infusion-site pain (29%), and dizziness (13%). All were mild.
What’s the takeaway?
FREEDOM-HF is less about “is SC equal to IV?” and more about “can we safely discharge the right patient with SC diuresis instead of admitting them for a short IV-diuretic stay?” In this (albeit, small and non-randomized) prospective vs matched-historical comparison, patients discharged with SC furosemide had a low 30-day HF hospitalization rate (1/24, 4.2%), lower mean HF-related costs versus controls, and improvements in symptoms/functional status (KCCQ-12, a HF health-status questionnaire) and natriuretic peptides (BNP/NT-proBNP). Adverse events were mostly mild and related to the infusion site.
Putting It All Together
It helps to separate “drug effect” from “care pathway.” Study #1 speaks to pharmacodynamic response. Over the first 6 hours, SC furosemide produced similar total urine output to IV dosing. Study #2, FREEDOM-HF, speaks to workflow. Using SC furosemide as part of an ED discharge plan for selected worsening-HF patients was associated with lower 30-day HF-related costs and improved patient-reported and biomarker outcomes compared with matched historical controls.
Taken together, these data support SC furosemide as an option for carefully selected patients when the goal is to achieve decongestion without a short inpatient stay, while recognizing the evidence base is still relatively limited and pathway selection matters.
And remember…send your de-identified intervention stories to steph@tldrpharmacy.com so we can give you a shoutout here on tl;dr! (Image)
