
The 30 mL/kg Sepsis Question: What Should Actually Be in the Bag?
A note from the tl;dr team: The content in this post has been reviewed and updated in accordance with the 2026 Surviving Sepsis Campaign (SCC) guidelines to ensure alignment with current evidence and best practices.

Since we’re on the topic of long-standing debates, what do you think Fred and Barney would say about colloids vs crystalloids…
Joe’s Note: This question has been debated for decades. Everyone knows fluid resuscitation is the first step in treating hypotension in patients with septic shock. Everyone remembers to give 30 mL/kg of fluids. But what should actually be in the bag remains a topic of debate. (Image) There are so many options to choose from…
For starters, you have to pick between colloids and crystalloids. And even if you decide on the type of fluid, you still have tons of options to choose from. From the colloid family, you have albumin (most common), fresh frozen plasma (please no), dextran (also please no), and hydroxyethyl starch (most definitely no). From the crystalloid family, you have dextrose (please no), normal saline, lactated ringers (LR), and plasmalyte. With so many options to choose from, does one rule over the others?
Well folks, today we’re going to answer all questions related to fluid resuscitation in septic shock. By the end, we’re going to figure out which fluid is king above all. And on the way, we’re going to debunk several myths regarding fluids and sepsis. So strap in and enjoy the ride.
P.S. Here’s a sneak peek of our roadmap for everything that we’re going to cover today:
Which is better: crystalloids or colloids?
Battle of the crystalloids: balanced crystalloids vs. normal saline
Does lactated ringers solution increase serum lactate?
Also one more thing. We’re not going to cover other aspects of sepsis in this post. We’re just focusing on fluid resuscitation. But lucky for you, take a look here if you need a refresher on everything you need to know about sepsis and septic shock. And if you want even more in-depth material, check out our sepsis cheat-sheet and antibiotic pocket guide :).
What is the Difference between Crystalloids and Colloids?
Great question. If you want an in-depth review of fluids, give this post a read. But if you want a quick summary, then keep on reading.
Long story short, colloids and crystalloids differ in their composition and volume expansion. Colloids are composed of large molecules that remain in the intravascular space due to high oncotic pressure. On the other hand, crystalloids are composed of small dissolved electrolytes or molecules that freely cross capillary membranes. As a result, only 10-25% of crystalloids remain intravascularly compared to ~100% of colloids. Let’s go over the numbers.
How much of the fluid stays in the intravascular space?
Crystalloids
Dextrose: ~10%
Normal Saline: ~20-30%
Lactated Ringers: ~20-30%
Plasmalyte: ~20-30%
Colloids
Albumin: ~100%
Dextran: ~100%
Starch: ~100%
Fresh Frozen Plasma: ~100%

Is this really what you want to do when you give a patient fluids?
Let’s put these numbers into perspective. If we give a patient 1 liter of normal saline, approximately ~250 mL will stay in the vascular space while the rest leaks out into the extravascular space. On the other hand, if we give a patient 1 liter of albumin, then almost the entire liter will stay in the intravascular space. Considering septic patients are volume depleted, we generally want to maintain as much fluid in the intravascular space to improve blood pressure. (Image)
So technically, colloids sound like they would be a better option, right? Keep on reading.
Colloids or Crystalloids for Septic Shock?
When it comes to medical debates, primary literature rules all. To avoid any bias, we’re going to review the guideline recommendations and the studies. The most popular studies comparing crystalloids versus colloids in sepsis include the SAFE trial, ALBIOS trial, CRISTAL trial, and the 6S and CHEST trials. Let’s go over them one by one. I don’t want to bore you to death so I will give a very quick and simplified summary of each study. However, I will link each study in case you’re a nerd like me and want to read more.
The SAFE Trial (Saline vs Albumin Fluid Evaluation, 2004)
This landmark trial randomized 6,997 critically ill adults to receive either 4% albumin or 0.9% saline for fluid resuscitation. Overall mortality was similar between groups (20.7% for albumin vs 20.8% for saline, P=0.87). In the predefined subgroup of 1,218 patients with sepsis, there was a trend toward lower mortality with albumin (30.7% vs 35.3%, P=0.09), though this did NOT reach statistical significance.
The ALBIOS Trial (Albumin Italian Outcome Sepsis, 2014)
This trial enrolled 1,818 patients with sepsis or septic shock and compared 20% albumin plus crystalloids versus crystalloids alone. The trial found no difference in 28-day mortality (RR 1.0, 95% CI 0.87-1.14) or 90-day mortality (RR 0.94, 95% CI 0.85-1.05). A post hoc analysis suggested potential benefit in the septic shock subgroup (RR 0.88, 95% CI 0.77-0.99), though the interaction test was not significant (P=0.19). Albumin resulted in higher blood pressure, higher static filling pressures, and lower net fluid balance.
The CRISTAL Trial (Colloids vs Crystalloids for the Resuscitation of the Critically Ill, 2013)
This multicenter trial randomized 2,857 adults in hypovolemic shock (including sepsis) across 57 ICUs to colloids (albumin, gelatin, or hydroxyethyl starch) versus crystalloids. The trial found no difference in 28-day mortality or renal outcomes between groups, with consistent treatment effects across diagnostic subgroups including sepsis, trauma, and other causes of shock.
The 6S Trial (Scandinavian Starch for Severe Sepsis/Septic Shock, 2012)
This trial of 804 patients with severe sepsis compared 6% hydroxyethyl starch (HES) 130/0.42 versus Ringer’s acetate and found increased 90-day mortality with HES (51% vs 43%, P=0.03). HES also increased the incidence of acute kidney injury (34.9% vs 22.8%, P=0.002).
The CHEST Trial (Crystalloid vs Hydroxyethyl Starch, 2012)
This trial of 7,000 ICU patients compared 6% HES 130/0.4 versus saline and found increased need for renal replacement therapy with HES (7.0% vs 5,8%, P=0.04). In the subgroup of 1,921 patients with sepsis, mortality was not significantly different but trended higher with HES (25.4% vs 23.7%, RR 1.07, 95% CI 0.92-1.25).
Alright, that's a lot of studies. What are the key takeaways, tl;dr style?
Mortality was similar in patients that received crystalloids versus albumin.
While there was no statistical significance in hemodynamics, patients that received albumin trended to better blood pressure, static filling pressure, and lower net fluid balance.
Hydroxyethyl starch (HES) is a horrible colloid and had higher mortality and need for renal replacement therapy compared to crystalloids. (Image)

Now let’s review the guidelines. The Society of Critical Care Medicine (SCCM) and Infectious Diseases Society of American (IDSA) recommend the following:
For adults with sepsis or septic shock, we “recommend” using crystalloids as first-line fluid for resuscitation
For adults with sepsis or septic shock, we “suggest” using crystalloids alone over crystalloids with supplemental albumin for fluid resuscitation
For adults with sepsis or septic shock, we ‘recommend against” using starches for resuscitation
For adults with sepsis and septic shock, we “suggest against” using gelatin for resuscitation
Their rationale? Crystalloids are preferred based on the absence of clear benefit from colloids compared to crystalloid solutions, combined with crystalloids being inexpensive and widely available.
Final Take: Crystalloids are recommended over colloids because they’re equally efficacious, have lower side effects, are much cheaper, and are more readily available.
Battle of the Crystalloids: Balanced Crystalloids vs. Normal Saline
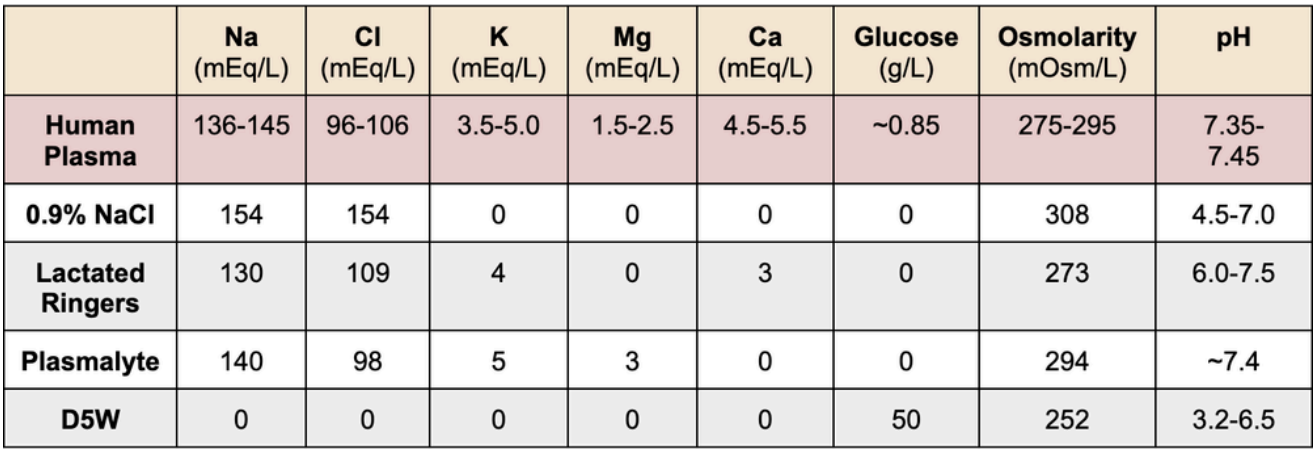
Okay we now know to use crystalloids over colloids. On to the next step. Which crystalloid? Our options include dextrose, normal saline, and balanced crystalloids such as lactated ringers and plasmalyte. In case you need a refresher on what’s in each crystalloid, take a peek below.
Let’s start with dextrose. Unlike the other crystalloids, only ~10% of dextrose stays intravascularly. So if we give 1 L of D5W, only ~100 mL will stay intravascularly while the rest leaks out. Obviously that’s not a favorable outcome considering we want as much fluid to stay intravascularly as possible to bring up that blood pressure.
In addition, dextrose contains no electrolytes and is therefore a hypotonic fluid. Large volumes of dextrose are going to plummet patients’ serum electrolytes and cause more harm than good (in addition to skyrocketing their blood sugar). So given all these points, dextrose should NOT be used for fluid resuscitation in septic patients.
On to normal saline versus balanced crystalloids. This is where the debate is. Just like we did before, we’re going to review the literature that shaped guideline recommendations.
This single-center, cluster-randomized, multiple-crossover trial enrolled 15,802 critically ill adults, including 1,641 patients with sepsis. The overall trial showed that balanced crystalloids reduced the composite outcome of death, new renal replacement therapy (RRT), or persistent renal dysfunction (14.3% vs 15,4%, P=0.04). In the sepsis subgroup specifically, 30-day in-hospital mortality was significantly lower with balanced crystalloids (26.3% vs 31.2%, P=0.01). The sepsis subgroup also showed reduced major adverse kidney events and increased vasopressor- and RRT-free days.
This Brazilian trial enrolled 10,520 critically ill adults and found no difference in 90-day mortality between balanced crystalloids and saline overall (26.4% vs 27.2%, adjusted HR 0.97, 95% CI 0.90-1.05). Among patients with sepsis, 90-day mortality was 46.7% with balanced crystalloids versus 49% with saline, which is not statistically significant.
This trial of 5,037 critically ill adults found no difference in 90-day mortality between balanced crystalloids and saline (21.8% vs 22.0%). Among patients with sepsis, mortality at 90 days was not significantly different between groups.
The CLOVERS Secondary Analysis (2025)
This recent analysis of 1,563 patients with sepsis-induced hypotension found that initial fluid resuscitation with lactated ringers solution compared to normal saline was associated with lower mortality (12.2% vs 15.9%, adjusted HR 0.71, 95% CI 0.51-0.99, P=0.043) and more hospital-free days. Patients receiving saline had higher chloride and lower bicarbonate levels.
While this trial enrolled 13,347 noncritically ill adults in the emergency department, it showed that balanced crystalloids resulted in lower major adverse kidney events (4.7% vs 5.6%, P=0.01) but no difference in hospital-free days. A secondary analysis suggested that early balanced crystalloid use in the ED may be particularly important for sepsis outcomes. A meta-analysis of 6,574 patients with sepsis from 5 RCTs showed no significant difference in mortality between balanced crystalloids and saline (31.3% vs 33.9%, RR 0.93, 95% CI 0.86-1.01), though Bayesian analysis suggested an 89.5% probability that balanced crystalloids decrease mortality.
Based on all this, the Surviving Sepsis Campaign 2026 guideline updates issued the following recommendation:
For adults with sepsis or septic shock undergoing initial resuscitation, we “suggest” using balanced crystalloids over 0.9% saline (normal saline)
Final Take: Balanced crystalloids are recommended over normal saline for fluid resuscitation in sepsis.
Does Lactated Ringer’s Solution Increase Serum Lactate?
The first step in our one-hour sepsis bundle is to collect a serum lactate to assess the severity of septic shock. In case you need a refresher, lactic acid (lactate) is a byproduct that is released when our tissues undergo anaerobic metabolism. If lactate is elevated, then it’s clear that we are not oxygenating our tissues appropriately (aka shock). Hence, we are forcing our organs to undergo anaerobic metabolism leading to increased serum lactate.
To reduce our serum lactate, we need to oxygenate our tissues appropriately so that our organs can go back to aerobic metabolism. How do we do that? Fluids, pressors, and stress-dose steroids.
So far we’ve come to the conclusion that balanced crystalloids (LR and plasmalyte) are the recommended fluids in sepsis. But LR stands for LACTATED Ringer’s. So could it worsen our serum lactate levels and make sepsis look worse than it actually is?

No. Lactated ringer’s has sodium lactate, NOT lactic acid. This is a completely different product and has absolutely no effect on our serum lactate levels. So please don’t avoid using LR in septic patients because you’re worried about increasing serum lactate. It’s just a myth folks. (Image)
P.S. If you want to read about other myths we debunk, check out our two posts here and here.
The tl;dr of Fluid Resuscitation in Sepsis
We’re going to keep it very very brief here. That’s the point of tl;dr anyway, isn’t it? So here you go:
Colloids are composed of large molecules that remain intravascularly due to high oncotic pressure.
~100% of colloids remain intravascularly.
Crystalloids are composed of small dissolved electrolytes or molecules that freely cross capillary membranes.
Only ~10-30% of crystalloid fluids remain intravascularly.
Crystalloids are recommended over colloids for fluid resuscitation in sepsis given equal efficacy, lower side effect profile, cheaper cost, and availability.
Hydroxyethyl starch should be avoided in sepsis due to increased mortality and need for renal replacement therapy when compared to crystalloids.
Balanced crystalloids (LR and plasmalyte) are recommended over normal saline for fluid resuscitation in sepsis given trends of better mortality, hospital-free days, and fewer adverse events.
LR has sodium lactate, NOT lactic acid. Therefore, use of LR is recommended in sepsis and has no direct correlation with increasing serum lactate.