
What Every Pharmacist Should Know about Febrile Seizures
Joe’s Note: I know I shouldn’t jump to conclusions, but I’m going to do it anyway. My guess is you probably learned about febrile seizures somewhere in school and again during your pediatric or ED rotation. Time has passed, and you forgot all about it. A few years later, you get married and decide to start a family (hooray!). You’re now a parent for the first time, and your newborn contracts an illness (that you probably brought home from work). And now you’re concerned for fevers.
Suddenly, those febrile seizures topic discussions you had a few years back start flowing through your head. You get nervous. (Image) Google and/or some form of AI become your best friend as you search:
“What is febrile seizure?”
“What temp should I be concerned about for febrile seizures?”
“How do I treat febrile seizures?”
“Should we go to the ED?”
“Is my infant at risk for febrile seizures?”
“Can I prevent a febrile seizure?”

The new parent Google search rabbit hole… been there.
Okay maybe that’s not your story, but it is mine. So, to spare you the anxiety that I had to go through, I decided it would be good to write about febrile seizures and prepare all the new parents out there. If you want the answers to those questions above, keep on reading!
What is a Febrile Seizure?
As the name suggests, febrile seizures are generalized seizures that occur in febrile (fevering) pediatric patients. They are typically seen in children between the ages of 6 months to 5 years and occur with a fever ≥ 100.4℉. And in case you need a refresher on normal infant temperature ranges, take a look below.
Oh and one more thing. Rectal measurement is the gold standard for accuracy in children under 3 years old since it provides the most reliable core body temperature.
Normal Temperature Range (rectal): 97.7℉ to 99.5℉ (36.5℃ to 37.5℃)
Low-Grade Fever (rectal): 100.4℉ to 102℉ (38℃ to 39℃)
Moderate Fever (rectal): 102℉ to 104℉ (39℃ to 40℃)
High-Grade Fever (rectal): 103℉ to 104℉ (39℃ to 40℃)
Very High/Dangerous Fever: >104℉ (>40℃)
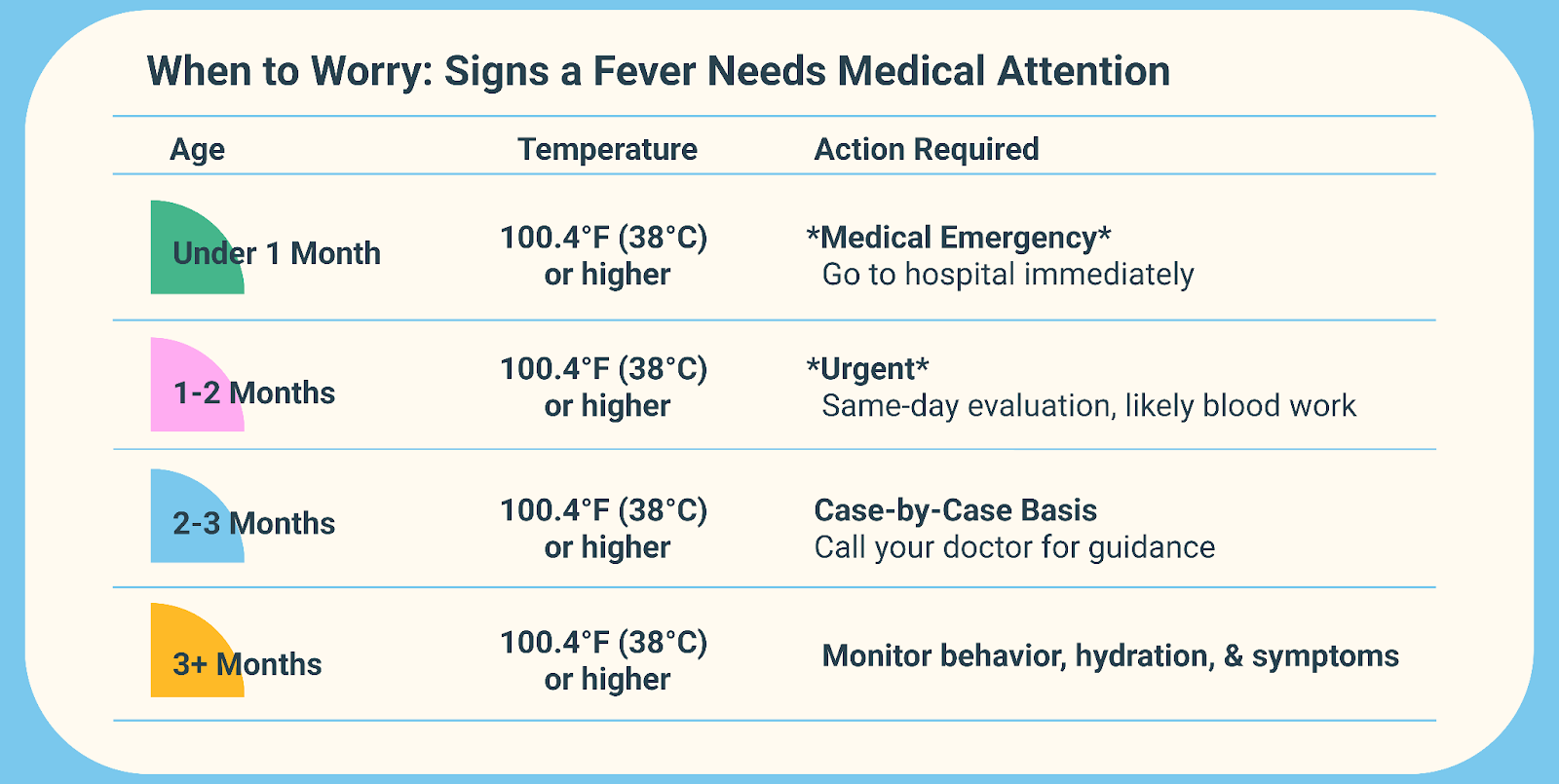
Now it’s also a little tricky because age plays into urgency as well. For example, a temperature of 101℉ in a 4 year old may not make you blink more than to say, “Oh hun, you’re probably coming down with something.” (And then you feel dread wash over you because you know you’re next on the list of whatever plague your dear sweet Petri dish has brought home…) But in a newborn, that same temperature is actually a medical emergency that warrants getting to a doctor ASAP. Check out this chart to see how not all ages are created equally when it comes to fever:
What Causes a Febrile Seizure?
Not to beat a dead horse but the straightforward answer is fevers ≥ 100.4℉ (38℃). And yes, even low-grade fevers can induce seizures in kiddos. (Comforting, right?) That being said, I think it’s important to talk about what DOESN’T cause febrile seizures.
This type of seizure is generally not neurogenic in nature. Meaning that it’s not associated with a central nervous system infection or any other known seizure-provoking etiology, such as electrolyte imbalance, hypoglycemia, or substance abuse.
Risk factors for febrile seizures include existing neurologic impairment, the presence of a viral infection, a family history of seizure, developmental delay, decreased serum zinc and iron levels, and maternal smoking and stress. Essentially, this seizure is caused by febrile illness NOT related to the CNS and does not meet criteria for other acute symptomatic seizures.
Got it? Great, moving on.
Febrile seizures are divided into 2 main categories: simple febrile seizures and complex febrile seizures. Let’s compare:

In general, simple febrile seizures are significantly more common than complex febrile seizures (phew). In fact, simple febrile seizures account for roughly 65-90% of all cases. That being said, simple febrile seizures should not be taken lightly. If not appropriately treated, they manifest into complex and even febrile status epilepticus. We’ll get more into treatment in a little bit. But for now, let’s talk about the pathophysiology of febrile seizures.
Patient-Friendly Pathophysiology of Febrile Seizures
Seizures are so complex, and I’m definitely not smart enough to get into the nitty gritty details of generalized seizures. So to spare you the medical jargon, I decided it would be best to give a very basic patient-friendly explanation of what happens during febrile seizures.
It typically all starts with some form of viral infection. To fight the infection, our immune system releases a bunch of cytokines (interleukins, interferons, TNF, etc), which results in a fever. Why does our body purposely increase our internal temperature?
Because inducing a fever creates an inhospitable, high temperature environment for pathogens, while simultaneously accelerating the immune system’s response. Fevers boost the production and efficiency of white blood cells, enhance the release of heat-shock proteins to aid immune cell trafficking, and speeds up metabolism for faster tissue repair. Pretty neat right?
In a mature fully developed brain, low-grade fevers are great and dandy since they can help fight infection and boost repair. But the young brain of infants and toddlers is not fully developed. These kiddos have more excitatory signals and less mature inhibitory control. And while fevers may help fight the infection, they also make neurons fire faster, leading to increased metabolic demand in brain cells.
Think of it as a car with a strong gas pedal but weak brakes. Or an overly sensitive smoke alarm that goes off with any heat rise, even though there isn’t a dangerous fire. (Image)
So yes, while fevers may fight infection, they also can cause neuronal excitement leading to unwanted seizures in young patients.
How to Treat Febrile Seizures?
Yay, we’re at the fun part now :). Before we get into the treatment, I want to give a very important disclaimer. The majority of febrile seizures are self-limiting and treatment mostly focuses on managing fever and preventing injury/recurrence. Most febrile seizures resolve spontaneously and return to baseline is quickly achieved without the need for acute intervention.
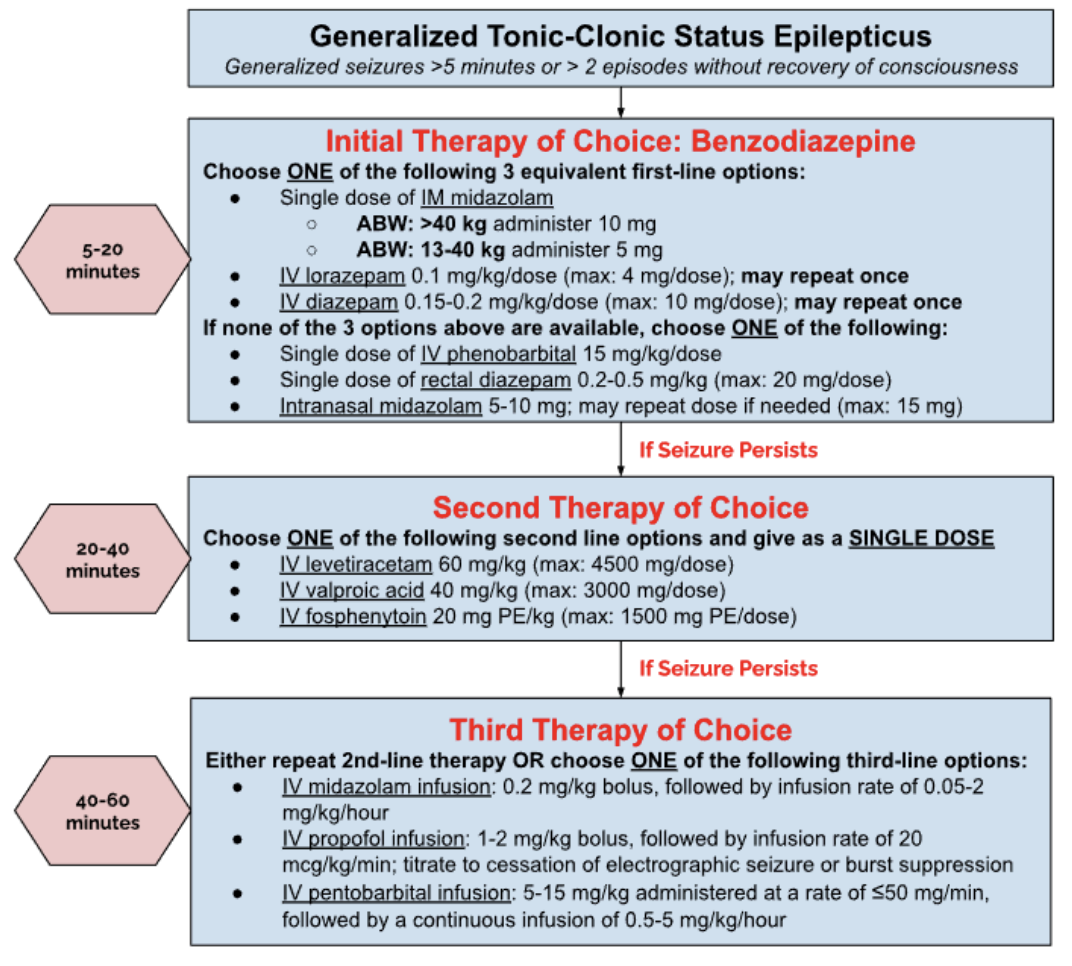
That being said, that’s not the case for every single patient. If a febrile seizure persists for longer than 5 minutes, emergency rescue therapy is needed. Luckily, treatment is the same as for status epilepticus. We’re not going to go super in-depth on the treatment of status epilepticus since we have a whole article about it here. But, to prevent you from having to click back and forth between the two articles, here is a step-wise approach I made for the treatment of acute status epilepticus:
The Role of Preventative Therapy - Anticonvulsants
I know. Logically speaking, if someone (especially a pediatric patient) experiences a febrile seizure, you’d assume that chronic antiepileptic medication would be needed to help prevent recurrence. While it sounds like a genius plan, literature would recommend otherwise.
Why? Great question.
Let’s take a step back and go back to the basics. When we treat any disease state, it’s vital to weigh the risks versus benefits of starting therapy. All meds come with unwanted side effects/adverse events. It’s impossible to avoid this. And when the benefits of treating a disease outweigh the risks, treatment is appropriate. But when the risks outweigh the benefits, then treatment is generally NOT recommended.
Now let’s take this concept and apply it to febrile seizures. Like we talked about earlier, febrile seizures have an excellent long-term prognosis with no evidence of causing structural brain damage, cognitive impairment, learning problems, or increased mortality. I’ll let the numbers speak for themselves.
The negatives first. Approximately 3-6% of children with febrile seizures will develop epilepsy later in life. That’s fairly significant tbh.
But many trials have been conducted to see if chronic antiepileptic therapy after a febrile seizure helps prevent the development of epilepsy. And the overwhelming answer is no, they don’t.
Now let’s look at the other side. Not only do antiepileptics NOT prevent the development of epilepsy in patients with a febrile seizure, but they also come with a handful of unwanted side effects. Specifically, it is estimated that phenobarbital and valproic acid cause adverse events in up to 30% of children, including behavioral problems and lower comprehension scores. Phenobarb and valproic acid are some of the more toxic antiepileptics, but the point remains true for all anticonvulsants.
As you can see, the risks of chronic antiepileptic therapy outweigh the benefits of preventing the development of epilepsy in patients that experience a febrile seizure. So please, do NOT start chronic seizure meds for these little kiddos.
The Role of Preventative Therapy - Antipyretics
Alright, on to our next med class. This one's a little more iffy in my opinion. For starters, the main antipyretics we’re talking about here are acetaminophen (most common) or ibuprofen (if >6 months old). On paper, it makes perfect sense. Viral infection causes fever, and fever causes seizure. So why not give an antipyretic to reduce/prevent that fever to avoid a seizure?
Because evidence shows that routine antipyretic use does NOT prevent febrile seizures during fever episodes.
A 2021 systematic review found no evidence supporting antipyretic prophylaxis for preventing seizures in distant fever episodes (odds ratio 0.92; 95% CI 0.57-1.48). Similarly, randomized controlled trials of ibuprofen showed no difference in recurrence rates compared to placebo, with 2-year recurrence probabilities of 32% versus 38% respectively. One recent randomized controlled trial suggested that rectal acetaminophen may reduce seizure recurrence within the same fever episode (9.1% recurrence with acetaminophen versus 23.5% in controls). However, this represents very limited evidence, and the systematic review examining this question concluded there is insufficient support for routine use even during the same illness.
Because of this overwhelming data, The American Heart Association and American Red Cross guidelines explicitly state that fever treatment can help children feel better but will not prevent subsequent seizures. The American Academy of Pediatrics similarly concluded that the risks and potential side effects of prophylactic antipyretic therapy do not justify their use for seizure prevention, as they don’t demonstrably improve long-term outcomes.
So what’s the overall consensus for use of antipyretics?
In general, antipyretics should be used on standard indications for comfort, NOT for seizure prophylaxis. Having a viral infection sucks, and these kiddos feel poopy. While acetaminophen or ibuprofen won’t necessarily reduce the risk for seizures, they definitely can help the child feel more comfortable.
So, What Can We Do for Febrile Seizures?
Truthfully, not much. Obviously if the febrile seizure escalates into status epilepticus, then rescue therapy is needed. But for the majority of cases, these seizures will resolve on their own, and supportive therapy remains the mainstay of management.
What you can do is provide parental education. It is important to emphasize the excellent prognosis, low risk of epilepsy brain injury, and practical guidance on home seizure management. Families should be provided with emergency contact information and reassurance about the benign nature of febrile seizures.
Oh and one more thing. Don’t forget to treat the underlying cause. Why is the patient febrile to begin with? Is it an infection, is it a recent immunization, are they dehydrated, etc? If we treat the underlying cause, we treat the fever and prevent the seizure. Pretty cool, right?
Tl;dr of Febrile Seizures
We went over a lot of information today. Incase you skipped all my beautifully written paragraphs above and want a quick tl;dr version, then please see below:
Febrile seizures are generalized seizures that occur in febrile (fevering) pediatric patients. They are typically seen in children between the ages of 6 months to 5 years and occur with a fever ≥ 100.4℉.
Febrile seizures are either simple or complex depending on duration, persistence, and recurrence.
The young undeveloped brains of infants and toddlers have more excitatory signals and less mature inhibitory control, leading to increased seizure risk.
The majority of febrile seizures are self-limiting, and treatment mostly focuses on managing fever and preventing injury/recurrence. If a febrile seizure persists for longer than 5 minutes, emergency rescue therapy is needed (please see picture above regarding the treatment of complex febrile seizures).
Febrile seizures have an excellent long-term prognosis with no evidence of causing structural brain damage, cognitive impairment, learning problems, or increased mortality.
Chronic (long-term daily) anticonvulsants are NOT recommended to prevent febrile seizures because the risks outweigh the benefits.
The American Academy of Pediatrics states that antipyretics should be used on standard indications for comfort, NOT for seizure prophylaxis.
Parental education, supportive care, and treatment of the underlying cause is the cornerstone for prevention and management of febrile seizures.