
When Good Drugs Go Bad: Acetaminophen Toxicity
Steph’s Note: We return this week with Dr. Josef Nissan, who recently provided us with the long-awaited, much-anticipated article on vasopressors as well as a mighty fine overview of heparin-induced thrombocytopenia. He’s here this week to educate us on a household drug name: acetaminophen. Who doesn’t have some sort of acetaminophen somewhere at home? Whether it’s Nyquil, some OTC headache concoction, or just plain old Tylenol, this easily-accessible medication is ubiquitous - but far from harmless! Time to learn what happens when a good drug goes bad…
If you’re looking for a handy guide to carry around with you when you’re covering the ICU/ED, check out our Pocket Guide to Pharmacotherapy Management of Acute Medical Emergencies. It’s 50+ pages of concise, practice-relevant critical care goodness that fits inside your white coat pocket.

(Image)
I once read online that I should crack a joke to begin an article to really “grab” the reader in. So here’s a low-quality meme…
Now that I have “grabbed” your attention, let’s talk about acetaminophen.
Acetaminophen (as you probably already know) remains one of the most accessible and commonly used medications in the United States. More than 60 MILLION Americans consume acetaminophen on a WEEKLY basis. Acetaminophen overdose accounts for over 60,000 EMERGENCY ROOM VISITS YEARLY, and acetaminophen toxicity is the SECOND most common cause of LIVER TRANSPLANTATION worldwide.
Am I being extra dramatic with all my capitalized words? Yes. But is this a really important topic that I think every healthcare provider should be comfortable with? Absolutely.
Back to Acetaminophen Basics
Let’s start with the basics. Acetaminophen is both an analgesic (pain reliever) and an antipyretic (fever reducer). While not fully understood, the analgesic effects are believed to be due to the activation of the descending serotonergic inhibitory pathways in the central nervous system. On the other hand, the antipyretic effects are believed to be produced from the inhibition of the hypothalamic heat regulating center.
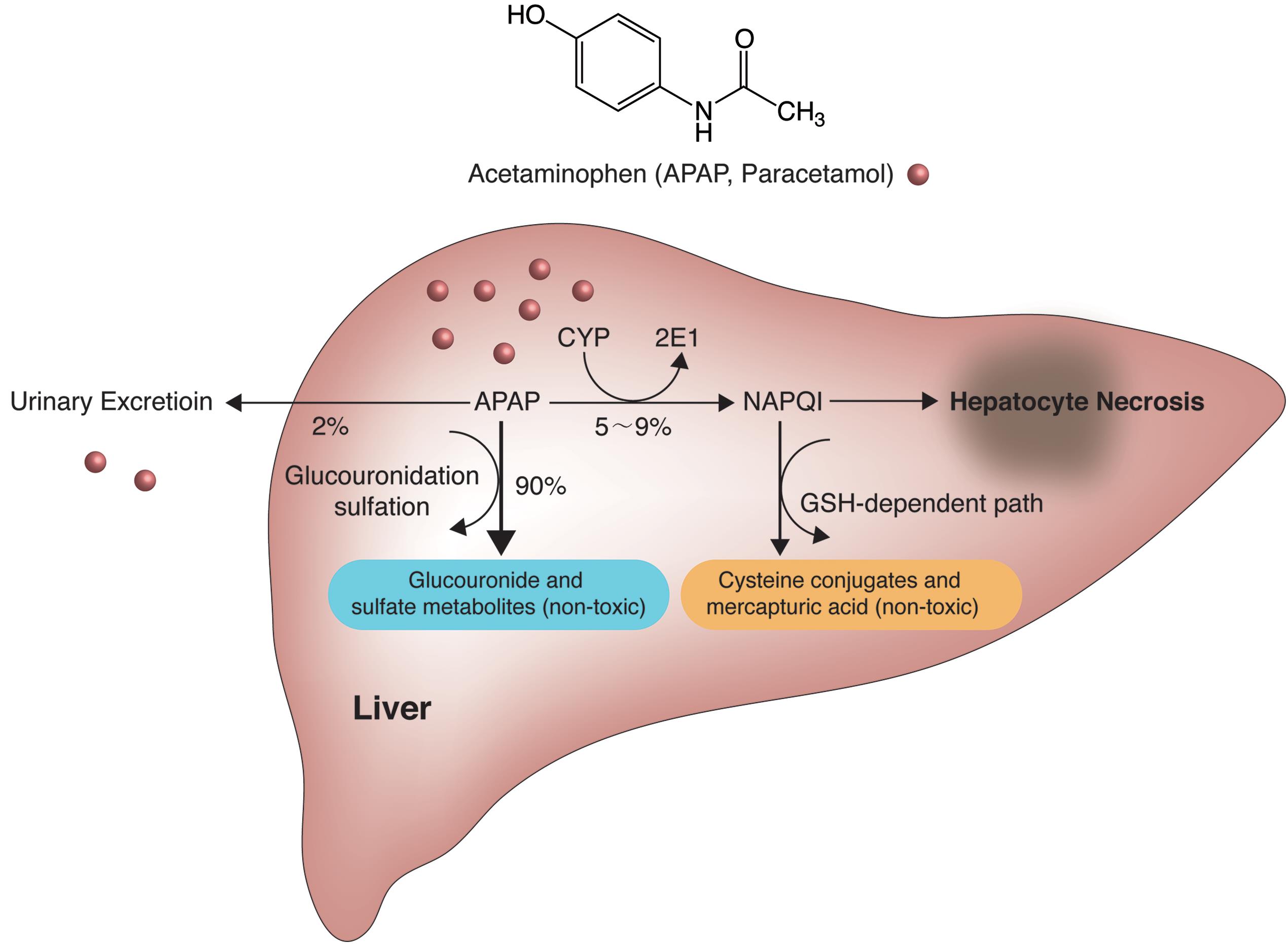
The recommended HEALTHY ADULT daily dose of acetaminophen is 650-1000 mg every 4 to 6 hours, not to exceed 4 grams/day. Acetaminophen has a fairly rapid onset of action in ~1 hour with a half-life of about 2-3 hours. At a normal therapeutic dose, acetaminophen is primarily metabolized by the liver to sulfate and glucuronide conjugates, while a SMALL amount is metabolized by CYP2E1 to a highly reactive intermediate, N-acetyl-p-benzoquinone imine (NAPQI).
Don’t you just love pharmacokinetics?
Pathophysiology of Acetaminophen Toxicity
Now that we’ve gone over the basic pharmacokinetics of acetaminophen, let’s talk about the pathophysiology of acetaminophen toxicity. To get a better understanding, let’s apply a clinical case. I want to feel special so I am going to use myself as the patient in this case.
Acetaminophen Case #1
Patient JHN (me, obviously) took the recommended acetaminophen dose for the day. My body primarily metabolizes that dose in the liver through glucuronidation and sulfation. When acetaminophen is metabolized by the glucuronidation and sulfation pathways, it produces NON-TOXIC METABOLITES that can then be excreted out of the body through the urine.
No harm here.
Acetaminophen Case #2
Patient JHN (me, again) accidentally took more than the daily recommended dose of acetaminophen :(. The glucuronidation and sulfation pathways activate to begin metabolism of the acetaminophen. However, since I took too much acetaminophen, those pathways become overworked and saturated. They no longer are able to keep up with all that extra acetaminophen in my body.
As a result, my body will begin to break down the excess acetaminophen by increasing the activity of cytochrome P450. And THERE lies the problem.
When acetaminophen is broken down by CYP450, it produces a HIGHLY REACTIVE AND TOXIC METABOLITE called N-acetyl-p-benzoquinone imine (NAPQI). NAPQI reacts with my liver cell proteins, causing hepatic necrosis (breakdown of liver cells).
That, my friends, is how high doses of acetaminophen cause liver toxicity. Here’s a nice picture to sum it all up for you visual learners:

GSH = glutathione = the key to converting toxic NAPQI into non-toxic metabolites so it doesn’t wreak havoc and kill hepatocytes (Image)
Signs and Symptoms of Acetaminophen Toxicity
Clinical symptoms of an acute acetaminophen toxicity are strongly dependent on two things: time since ingestion and amount consumed. Some patients may be completely asymptomatic, while others might go into full-blown liver failure. Let’s review.
Within the first several hours post ingestion: the patient is probably asymptomatic but may have some nausea and vomiting.
Within 24 to 72 hours post ingestion: abdominal pain, nausea, and vomiting are likely to occur. Some abnormalities in the patient’s liver function tests may start to arise during this period.
Within 3 to 4 days post ingestion: THIS is the time frame in which liver functions tests will be elevated. Some jaundice (yellowing of the eyes and skin caused by excess serum bilirubin), increased bleeding, and worsened nausea/vomiting may also develop.
Five or more days post ingestion: The patient will either recover or experience full-blown liver failure.
BTW - This is a lot of info. We’ve got a downloadable (and printer-friendly) PDF of this article you can download here. It’s perfect for offline reading and handwritten notes.
Acute Management of Acetaminophen Toxicity
There are two main options for the treatment of acetaminophen toxicity/overdose.

Apparently there is a trend about using activated charcoal for teeth whitening, so there are far more image options on Google for “charcoal mouth” than I would have ever imagined. (Image)
The first is activated charcoal, which is given by mouth at a dose of 1 g/kg (maximum dose: 50 grams). Now if you’ve never seen this stuff, let me tell you - it looks like someone took a handful of your campfire charcoal and pulverized it into a slurry. Steph can attest to how it tastes (thanks to a fun class in pharmacy school) - gritty. Bonus, it leaves your mouth black as night and feeling like you ate some topsoil out of the yard. But hey, better than liver failure, eh?
So how can a variation of such a common substance as charcoal treat acetaminophen toxicity?

For the visual folks out there… (Image)
After ingestion, charcoal is not absorbed from the GI tract. Rather, it hangs out there and adsorbs (not absorbs, adsorbs!) acetaminophen in the stomach. What is this adsorption of which we speak?
According to the Oxford Dictionary, to adsorb is to “hold (molecules of a gas or liquid or solute) as a thin film on the outside surface or on internal surfaces within the material.” So the activated charcoal attempts to suck up as much of the acetaminophen onto its surfaces as equilibrium will allow. This prevents the acetaminophen from being absorbed from the GI tract, thereby limiting the amount of acetaminophen that reaches the bloodstream.
Fun fun…the charcoal also induces vomiting, which again, leads to less acetaminophen being absorbed from the GI tract and entering the bloodstream.
In reality, activated charcoal is rarely ever used because its effectiveness is so time dependent. Because its actions are local to only acetaminophen still sitting in the stomach, it’s really only an option for patients who present within ONE HOUR (maaaaybe TWO, according to some) after acetaminophen ingestion. Otherwise, you’ve likely missed the boat, and the activated charcoal won’t help acetaminophen already absorbed into the bloodstream.
Now how often do we know an exact time of ingestion or overdose? And would you be willing to gamble someone’s liver and bet that you’re within the 4 hour window to use this medication if you’re not ABSOLUTELY sure?
Yeah, me neither. Hence, it’s rarely used. But it’s still good to know about and have in your back pocket in case it’s a witnessed ingestion within the appropriate timeframe.
On to option #2, which is N-acetylcysteine, or NAC. While this medication has various properties that have been exploited to treat patients (including as an inhaled mucolytic!), in cases of acetaminophen toxicity, we are using it for its ability to restore hepatic glutathione (GSH). Glutathione is made in the liver from three amino acids: glycine, cysteine, and glutamic acid, with the availability of cysteine thought to be the rate-limiting component of GSH synthesis. So, by supplementing NAC, the idea is to provide the rate-limiting cysteine that the body needs to make more GSH.
Remember, GSH is the king of antioxidants that helps to convert NAPQI into non-toxic metabolites so it can’t shift everything towards hepatic destruction. The non-toxic metabolites are then excreted out of the body, and no harm, no foul.
But without glutathione or not enough glutathione… no bueno.
N-acetylcysteine can be given either through the IV or PO route. However, IV administration is usually PREFERRED. (There are a couple reasons for this, but one of them is patient tolerance… As discussed, NAC contains cysteine, which is a sulfur-containing amino acid. Guess what sulfur smells like - rotten eggs and stink bombs. And again, as Steph can attest thanks to that class in pharmacy school, no matter what kind of beverage it’s mixed with and even if it’s covered with a lid, that awful smell still travels right up to the nose! Not great for an entire PO regimen.)
The IV protocol is a 20 hour treatment:
Loading Dose: 150 mg/kg (max: 15 g) infused over 1 hour
Second Dose: 50 mg/kg (max: 5 g) infused over 4 hours
Third Dose: 100 mg/kg (max: 10 g) infused over 16 hours
The PO protocol is a 72 hour treatment (rotten eggs for 72 hours!!):
Loading Dose: 140 mg/kg
Maintenance Dose: 70 mg/kg every 4 hours for a total of 18 doses
NAC is typically the first-line option for the treatment of acetaminophen toxicity. However, does every single patient that comes into the ED for taking too much acetaminophen need N-acetylcysteine? No, because a lot of times supportive care is all you need.
So how do we decide who to treat with N-acetylcysteine?
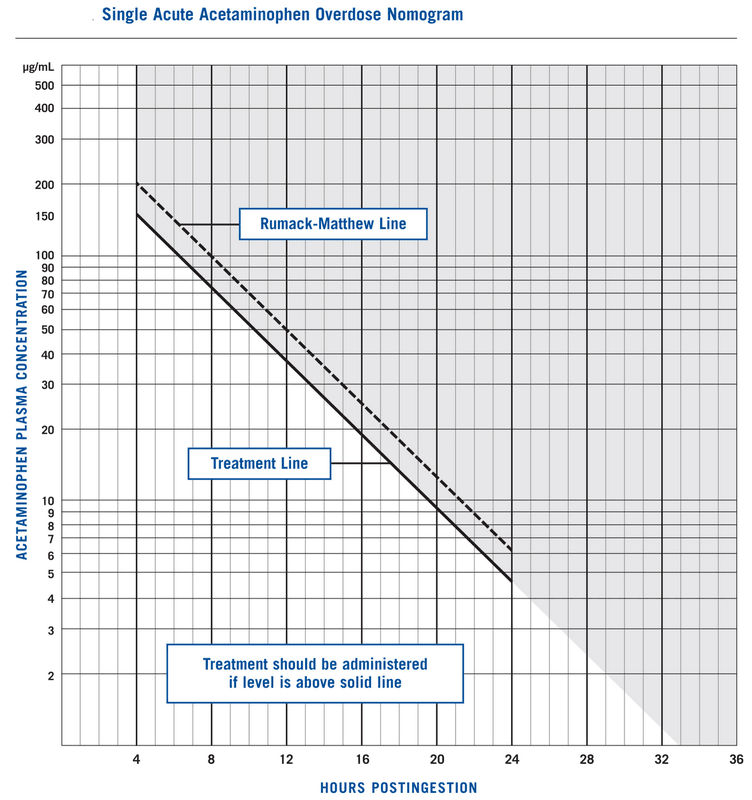
Well it’s easy. All you have to do is check the Rumack-Matthew nomogram. Let’s take a look.
The Rumack-Matthew Nomogram for Acetaminophen Toxicity

{kind=link}
{kind=link}
The treatment line (solid black) is placed 25% below the Rumack-Matthew line (dotted black) because this allows for a little more “wiggle room” for reported ingestion times. It essentially means more patients will receive treatment, so it’s more conservative in that we’re not gambling with someone’s liver. (Image)
{kind=link}
When trying to interpret the Rumack-Matthew nomogram to see who qualifies for treatment with N-acetylcysteine, you need to look at two main variables:
the number of hours post acetaminophen ingestion and
the acetaminophen plasma concentration.
Anything above the treatment line should be treated with N-acetylcysteine since there is a risk for possible hepatotoxicity. Anything below the treatment line typically does not require acute treatment with N-acetylcysteine.
Let’s go back to the original cases we discussed earlier to put this into perspective.
In the first case, patient JHN took the recommended daily dose of acetaminophen 7 hours ago. So let’s say you took a serum acetaminophen level, which resulted at 10 mcg/mL. To figure out if JHN has a risk for hepatotoxicity and needs N-acetylcysteine treatment, we will use the Rumack-Matthew nomogram.
At the 7 hour mark with an acetaminophen concentration of 10 mcg/mL, patient JHN is below the treatment line and therefore does NOT require acute treatment.
In the second case, patient JHN took more than the recommended daily dose of acetaminophen 20 hours ago. Let’s say his serum acetaminophen level resulted at 200 mcg/mL. Using the Rumack-Matthew nomogram, an acetaminophen level of 200 mcg/mL at the 20 hour mark is ABOVE the treatment line, and therefore this patient SHOULD be treated with N-acetylcysteine.
See, it’s pretty simple. As long as you have the time of ingestion and the serum acetaminophen level, then using the Rumack-Matthew nomogram to decide when to treat an acetaminophen overdose/toxicity is super easy. (Of course, when it gets hard is when you have no clue as to when the patient actually ingested the acetaminophen - either because they can’t or don’t want to tell you… This makes using the nomogram rather difficult!)
The tl;dr of Acetaminophen Toxicity and Overdose
Acetaminophen remains one of the most accessible and commonly used medications in the United States. This is a little scary since acetaminophen toxicity is the second most common cause of liver transplantation worldwide. At therapeutic doses, acetaminophen is primarily metabolized in the liver through glucuronidation and sulfation into NON-TOXIC metabolites that can then be excreted in the urine.
Supra-therapeutic doses of acetaminophen saturate the glucuronidation and sulfation pathways leading to an increase in CYP2E1 metabolism. Metabolism of acetaminophen by CYP2E1 produces a highly HIGHLY REACTIVE AND TOXIC metabolite called N-acetyl-p-benzoquinone (NAPQI).
NAPQI damages liver cell proteins causing hepatic necrosis and hepatotoxicity. Clinical signs and symptoms of an acute acetaminophen toxicity are variable and depend on the time since ingestion and amount consumed.
There are two main pharmacotherapy options for the management of acetaminophen toxicity: activated charcoal and N-acetylcysteine. Although activated charcoal may be an option for patients that present within FOUR HOURS post acetaminophen ingestion, preference is generally given to intravenous N-acetylcysteine.
The Rumack-Matthew nomogram can be used to determine which patients are at risk for hepatotoxicity. Treatment with N-acetylcysteine should be initiated for all patients above the treatment line in the Rumack-Matthew nomogram.
And there you have it! A rundown of some very serious complications from a readily available OTC therapy.