
The Real Deal on Penicillin Allergies
A note from the tl;dr team: This content was reviewed and updated in March 2026 to ensure accuracy and relevance
Steph’s Note: This week, we’re taking a detour into the world of antibiotics. Basically, this post is going to tell you how to be a pharmacy superhero. Not only are we going to introduce you to the Matrix theory of penicillin allergies, but we’re going to give you the skills to strategize targeted beta-lactam recommendations when others may write them completely off as options. (If you want another tool for antibiotic recommendations, don’t miss out on our ridiculously useful Antibiotic Cheat Sheet. And if you want an even more in-depth review of everything infectious disease, check out our Antibiotic Pocket Guide)

(Image)
Here to feed us the blue (or was it red?) pill to show us behind the beta lactam Matrix is Shelby Gross.
Shelby Gross, PharmD is finishing up her PGY-1 residency at University Medical Center New Orleans. She is a New Orleans native and graduated from Xavier University of Louisiana College of Pharmacy in New Orleans, LA. Her professional interests are primarily all things infectious diseases and antimicrobial stewardship, but she’s also interested in a little bit of everything. (Insert shameless Twitter plug - @shelbactam). Outside of pharmacy, she tends to her collection of succulent plants, spends time with family and friends, and enjoys traveling to explore new places. Post-residency, she plans on taking some time to catch up on sleep before embarking on the hunt for a clinical position.
Imagine you are taking a quiz during your Infectious Diseases block and you come across this question:
Which is NOT a cephalosporin class effect?
Penicillin allergy cross-reactivity
Kernicterus
Myelosuppression
Seizures

Ok, so we’re not taking you into an alternate universe with this post. But it may very well feel like it given the differences between what you learned in school and what we’re sharing here!
The correct answer choice is B. (Kernicterus is a unique effect with ceftriaxone, particularly when used in neonates.)
But what if I told you there was more than one correct answer choice here? Which would you think is most likely to also be correct?
*Cue dramatic music*
Although not by the technical NAPLEX study guide, answer choice A is also correct!
There are a lot of misconceptions surrounding beta-lactam and penicillin allergies. Universal cross-reactivity between beta-lactams (penicillins, cephalosporins, and carbapenems) is essentially an urban legend that we’ve all been taught by textbooks. I suppose now would be the best time for me to insert a disclaimer.
❗❗❗ DISCLAIMER ❗❗❗
If you’re taking any sort of board exam (i.e., NAPLEX, MPJE, etc.), you should definitely operate under the assumption that there is a one-size-fits-all cross-reactivity between all beta-lactams when selecting answer choices. But we’re going to shatter this textbook urban legend for practical, real-world practice purposes.
Alright, now that we’ve got that out of the way, let’s dive into a little background.
How many people have a penicillin allergy?
Approximately 10% of the population in the United States reports a drug allergy to beta-lactam antibiotics, making it the most commonly reported drug allergy nationwide.
I should place more emphasis here on “reported.”
That’s because it’s thought that over 90% of reported penicillin allergies are not actually true hypersensitivity reactions and likely represent something else, such as adverse effects or a symptom related to the infection being treated. This is one reason that a solid, thorough reconciliation of allergies should occur at the point of admission (ideally along with a medication reconciliation)! Sure, it’s great to have drug names listed in the chart allergy section, but it’s so much more helpful if additional questions are asked to characterize, “Well, what happened when you took this medication?” Ideally, each listed “allergy” should be further categorized as a true allergic reaction (e.g., hives, anaphylaxis) or an intolerance or adverse reaction (e.g., nausea, diarrhea, etc).
Honestly, you’ll probably find that most people love to tell a good medical story, and you usually get PLENTY of details about what happened when they took drug A.
In addition to many reported drug reactions not being true allergies, even many patients who have a confirmed IgE-mediated (Type I) hypersensitivity reaction do not remain susceptible to these reactions forever. Interestingly, the immune system sort of “forgets” to react once about 10 years have passed since exposure.
Why do we care so much about penicillin allergies?
Well, beta-lactam antibiotics are the drugs of choice for multiple infectious diseases. Research has shown that patients labeled with a penicillin allergy are more likely to have:
Prolonged length of hospital stay
Delayed empiric antimicrobial therapy by an average of 50 minutes
Toxicity associated with 2nd-line agents
C. difficile infection
Methicillin-resistant Staphylococcus aureus (MRSA) infection
Vancomycin-resistant Enterococcus (VRE) infection
Surgical site infection from using 2nd-line prophylactic agents
Treatment failure in gram-negative bacteremia
Increased mortality, especially in hospitalized cancer patients
Treatment failure, infection recurrence, and death in patients with methicillin-susceptible S. aureus (MSSA) bacteremia with alternative therapy (i.e., vancomycin)
I don’t know about you, but seems like a pretty influential list of reasons to get the allergy list clarified up front, doesn’t it?
Just a quick note. The information we’ll be discussing in this post only applies to IgE-mediated (Type I) hypersensitivity reactions (i.e., immediate, anaphylactic reactions) and should NOT be used to guide decisions for alternative therapy in patients with delayed hypersensitivity reactions (i.e., Stevens-Johnson syndrome [SJS], drug rash with eosinophilia and systemic symptoms [DRESS], toxic epidermal necrolysis [TEN], hemolytic anemia, serum sickness, etc.)
How do beta-lactam antibiotics cross-react?
At the beginning of my PGY-1 residency, I noticed that prescribers often called before placing orders for an antibiotic to ask if another beta-lactam would cross-react with a patient’s reported penicillin allergy. I also noticed that the central pharmacists verifying orders frequently received calls from prescribers to notify them of a documented penicillin allergy when orders were placed for a beta-lactam. I started wondering - if all beta-lactams have a warning, why would some agents cross-react and others not? Is there something that wasn’t part of my pharmacy school review on this subject?
If you’re rusty on your organic and medicinal chemistry, bear with me. We’ll be diving into the structural characteristics of these drugs for just a minute because it’s just that important.

Generic penicillin structure with the beta lactam ring in red. (Image)
Drugs within the beta-lactam class include penicillins, cephalosporins, carbapenems, and monobactams (i.e., aztreonam). They are bactericidal and work by inhibiting cell wall synthesis.
The beta-lactam structure mimics the D-Ala-D-Ala cell wall substrate used by transpeptidase enzymes (also known as penicillin binding proteins or PBPs) to form bonds between peptidoglycan chains during cell growth. By fooling PBPs, beta-lactams bind to and inhibit the active sites, preventing cell wall formation.
In addition to the core beta-lactam structure, each agent also has distinct side chains and side rings which offer different pharmacokinetic properties and different spectra of activity. (I know, I know, I promise we’re almost done with the medicinal chemistry review.) Regarding side chains, they can be found at two locations commonly called R1 and R2 on the beta-lactam ring.
The R1 side chains are the real culprits when it comes to allergic reactions. Particularly, the R1 side chain has been identified as the major cause of IgE-mediated (Type I) hypersensitivity reactions.

(Image)
In the top two figures in the image, we see the generic penicillin and cephalosporin structures, along with the location of the R1 side chain. Then, the remaining structures in the bottom portion of the graph are the different R1 side chains that can fill that spot. The drug names listed next to each R1 side chain image share identical or similar side chains with each other (similarity is indicated by an asterisk). The different font colors represent the class of penicillin or cephalosporin with the color codes defined as follows:
Blue = aminopenicillins
Orange = 1st generation cephalosporins
Green = 2nd generation cephalosporins
Purple = 3rd generation cephalosporins
Red = 4th generation cephalosporins
Gray = monobactam
So just to be clear - we are not matching R1 side chains based on matching drug colors in this chart!
From this, we can use the similarity of R1 side chains to sort of risk stratify the chance that a patient will experience a hypersensitivity reaction with another agent.
For example, if you have a patient with a documented anaphylactic reaction to ampicillin, would you feel comfortable recommending cephalexin as an alternative? Would cephalexin be an acceptable alternative in the setting of an anaphylactic reaction to penicillin?
Let’s look at an example.
In the image, cephalexin and ampicillin are listed next to two different R1 side chain images in the bottom left side of the table. They share a similar side chain to amoxicillin, cefadroxil, and cefprozil, as indicated by the asterisks next to their names (while amoxicillin, cefadroxil, and cefprozil are shown to share identical side chains). Ampicillin, cephalexin, and cefaclor share identical side chains (and similar to the previous cell, share similar side chains with amoxicillin, cefadroxil, and cefprozil, as indicated by the asterisks now next to these drugs).
Using this information, in the case of a documented anaphylactic reaction to ampicillin, I probably wouldn’t recommend cephalexin as an appropriate alternative given their identical side chains (increasing the likelihood for cross-reactivity).
In general, we consider the earlier cephalosporin generations as more likely to cross-react with penicillins. However, there is one exception to this early generation rule of thumb. Even though cefazolin is a first generation cephalosporin, it has a unique R1 side chain compared with all other beta-lactams. This means the chance for cross-reactivity between cefazolin and other beta-lactams, including penicillin or ampicillin, is slim to none. Think of the implications here…
How many times have you seen vancomycin prescribed for a straight-forward, fiery red cellulitis, only because the patient had a listed penicillin allergy? We can do better! What if that penicillin allergy was just some nausea? Or a forgotten or never known reaction when your 75 year old patient was a toddler? Using cefazolin instead of vancomycin means using a more targeted and effective therapy for the likely cellulitis pathogens, less pharmacist time to manage, decreased cost of serum drug levels, and potentially decreased risk of toxicities, simply by doing a more thorough assessment of allergies at the point of medication decisions. The power of side chains, at work!
On another note, in school, we all learn that aztreonam is the safe option for a patient with a documented, true penicillin allergy. Ironically, aztreonam and ceftazidime share an identical R1 side chain, meaning that it would not be the best option in a patient with a history of anaphylaxis to ceftazidime.
So, after all this talk about side chains, where does the beta-lactam ring come into play?
The short answer is that it actually hasn’t been implicated as a mechanism for allergic cross-reactivity, unlike side chains. Historically, the beta-lactam ring was thought to be the cause, but upon further research, it seems that the cross-reactivity can be attributed to similar R1 side chains. (Also, early manufacturing processes of cephalosporins may have resulted in contamination with penicillin, but this isn’t so much of an issue these days.)

Summary of cross-reactivity between beta lactam agents. (Image)
How Can I Check if Beta-Lactams Cross-React?
I feel like we’ve nerded out enough already with all this talk about chemical structures and R1 side chains. Now let’s put o-chem stuff aside for a second and talk about true clinical relevance. It’s good to understand the background of all this but it’s even more important to be able to apply it to your clinical practice.
To start, I want to share with you this table that I recommend you use for the rest of your pharmacy career. Print it out, save it, hang it up, keep it in your white coat, and maybe even in your car. This table will help you answer one of the most common questions you’ll get as a pharmacist: “can I use *insert beta-lactam antibiotic here* if my patient has a documented penicillin allergy”. Take a peek
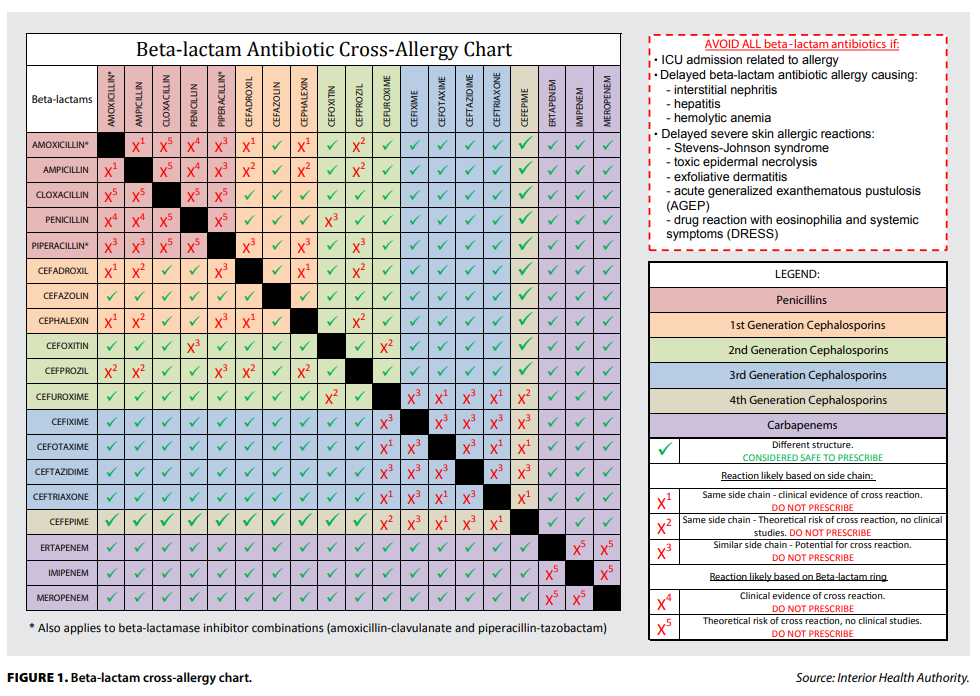
To use this table, all you have to do is line up the antibiotic in question with the allergy antibiotic. If there is a green check, then you can safely assume that these beta-lactams share different side chains and can be safely used with low/no risk of cross reactivity. If you see a red “X”, then you know to avoid the antibiotic in question given the higher risk for cross reactivity.
Let’s practice with a small case followed by two questions.
Case: SF is a 38-year-old female with no PMH who presents to your emergency department complaining of new onset lower leg swelling, tenderness, and warmth. The attending physician is concerned for cellulitis and would like to treat but is concerned about her documented penicillin allergy.
Question 1: Can cefazolin be safely used in this patient?
Question 2: Can cefoxitin be safely used in this patient?
Tl;dr answers: question 1 (yes), question 2 (no). It’s pretty straight forward. If you line up penicillin and cefazolin, you see a green check mark which means “good to go :)”. But if you line up penicillin and cefoxitin, you are welcomed with a big red X. Long story short, penicillin and cefazolin have different side chains while cefoxitin and penicillin share a similar side chain and cross reactivity is possible.
The tl;dr of penicillin allergies
Although one could argue that this is a lot of medicinal chemistry theory, it has been shown in ~real life~ that there is:
< 1% likelihood for cross-reactivity between penicillins and cephalosporins in those with patient-reported penicillin allergies,
< 2% likelihood for cross-reactivity between penicillins and cephalosporins in confirmed penicillin allergy cases, and
≤ 1% likelihood for cross-reactivity between carbapenems and any other beta-lactams.
So don’t write off the whole beta lactam class just because you see a listed penicillin allergy. It’s certainly worth the time to investigate deeper and do a little research into beta lactam side chains to see if there’s an option that may still cover the desired indication while minimizing the risk of a reaction. And if you ever feel stuck, make sure to use that table above. It’s a life savior.