
HIV Boot Camp: Background and Pathophysiology
Editor's note: To date, our most reader requested topic has been HIV. We've written a guest post at MedEd101 to cover the most NAPLEX-worthy testing points. But we thought we'd dig in a little further here. Over the next few weeks, we're posting a series called HIV Boot Camp. We'll shore up your HIV fundamentals. Then we'll breakdown each drug class piece by piece to highlight what you need to know.
You can get a downloadable (and printer friendly) PDF of the entire series here.
Part 1: Background and Pathophysiology
Background
HIV is a bastard. Let's just start right out with that. Although it's thought to have been around for decades, it didn't really "arrive" on the US scene until the early 1980s. It made it's first splash with strings of case reports involving healthy gay men getting a rare lung infection called Pneumocystis carinii pneumonia (PCP).
After about a year, with more cases of PCP mounting up, it was decided that something sexual must be transmitting this immune deficiency. It was considered an immune deficiency because PCP does not typically cause disease in healthy people.
So the super awesome and totally PC move was made to call this new syndrome "GRID." Gay-Related Immune Deficiency. Yep. That's what science decided.
Anyway, then some other stuff happened. We eventually started calling it Acquired Immunodeficiency Syndrome (AIDS). We learned that it was caused by a retrovirus named Human Immunodeficiency Virus (HIV). Getting diagnosed with the HIV was basically considered a death sentence. Tom Hanks won an Oscar. The Broadway musical "Rent" was made. Magic Johnson defeated the virus with cash. And eventually treatment advanced to present day where (if managed properly) HIV can almost be considered a chronic disease. Not too dissimilar from heart disease or diabetes.
As an interesting (to me) side note, HIV is one of the earliest retroviruses ever discovered. Our central dogma of biology clearly stated that the order of operations went from DNA to RNA to Protein. We had a hard time figuring out what HIV was because it went from RNA to DNA to RNA to Protein. More on that in a bit...
Pathophysiology
So what exactly does HIV do to the body?
Like other viruses, it hijacks your body's cells and turns them into virus factories. From the patient's perspective, it goes like this. You're exposed and nothing happens for about 10 days. The virus exposure most likely came from either unprotected sex or IV needle sharing. But it can also be transmitted vertically (mother to baby).
Anyway, you're feeling fine and then all of a sudden you're not. You have to leave work early because you've got a fever of 102 and you're all achy. Your head hurts. You're exhausted. Your face is flushed. There's a rash on your back and abdomen. Every time you swallow it feels like you're trying to get down a golf ball. You take Advil. It does nothing. You take Tylenol. It does nothing. You lay down on the couch and try to binge watch the new season of Unbreakable Kimmy Schmidt. But you can't focus. You throw up into the small bathroom trash can you placed by the couch. You have a hard time keeping down even gatorade and sprite.
Then you keep doing this for a full week or two.
You try going to a doctor. They run an influenza test (if it's in season) and find that it's negative. They tell you that you probably have the flu anyway. They say to keep up your fluid intake and to try to eat a soft diet of soups and broths.
Finally (thank God) it gets better. You start to feel normal again. You're exhausted and dehydrated, but your appetite comes back. You go back to work. And after another few days or so you start to feel like your old self again. You finally resume your social life and everything is right in the world again. You go on about your life for a few years with no real restrictions.
Then things start getting weird. You feel like you're constantly getting colds. You've been losing weight gradually for a few months. You've had bronchitis 3 times this year. Last month, you had an ear infection. A friggin' ear infection! What are you, 5 years old?! Finally on what feels like your 14th trip to the doctor, they take some blood and run some tests.
A day or two later, they call you and ask you to come into the office.
They sit you down on the exam chair with the disposable rolled out paper. And they tell you that you have HIV. Your CD4 count is 160. They want to send you to a specialty clinic to do some more tests and discuss treatment options.
So what's happening in the story above?
Once in the body, HIV burrows its little way into the cells of your immune system. Primarily, it goes into T lymphocytes (specifically, CD4+ T-lymphocytes), but it also can infect macrophages, dendritic cells and more. When it first causes infection, it spends some time under the radar replicating in these immune cells.
Eventually, the immune system catches on and gets pissed. It goes ape shit for a few weeks launching every countermeasure it can think of. Think "Independence Day" where we ineffectively send planes and even atom bombs up against the aliens to try to beat their superior technology.

The body develops antibodies to HIV. This is called seroconversion, and it's what the poor patient above was going through for 2 or 3 weeks feeling like he had the flu.
Then it enters a "clinical latency" phase that can last for years. Patient's are asymptomatic, but behind the scenes their CD4 counts are steadily dropping at a rate of about 200 cells/ml per year. Meanwhile, the number of HIV copies in the body is steadily increasing. On a graph, it looks like this:
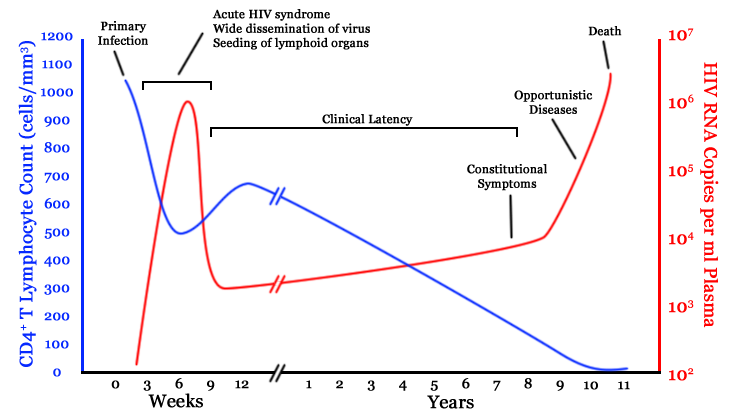
HIV Time Course. Image Source: Wikimedia Commons
Eventually, CD4 counts get so low that "weird diseases that don't infect healthy people" start showing up. These are the opportunistics such as PCP and MAC. Untreated, HIV is indeed a death sentence....but indirectly. It's normally a respiratory infection or similar that technically ends up "killing" the patient.
About that retrovirus bit from earlier...
We'll go into more specifics of the virus life cycle when we talk about the actual treatments for HIV. That way we can see what each drug class does to affect each stage of viral replication. But, we'd be remiss to not mention this one bit about retroviruses in general.
They mutate all the damn time.
Most known retroviruses (HIV included) use an enzyme called reverse transcriptase to break the central dogma of DNA to RNA to Protein. Reverse transcriptase is what converts RNA into DNA. It's also extremely error prone. It's like that friend you have that never has her shit together. She's always late. She's forgets to bring her pencil to class. She locks her keys inside her car. She's clutzy. She just spilled coffee on herself (again).
That's what reverse transcriptase is. Like your friend, reverse transcriptase means well. It tries to faithfully convert RNA to DNA with no mistakes and no hassle. But inevitably it always makes a mistake.
Why does this matter?
Because a virus that mutates all the damn time is a pain in the ass to treat. It quickly gains resistance to a given drug or a regimen. Meaning that even stable patients will periodically need to check their viral loads and CD4 counts. If either starts going in the wrong direction, then it's time to run another genotype to see if there's new resistance.
That's it for now. In Part 2 of HIV Boot Camp, we'll cover general treatment goals and considerations. This will give you a nice 10,000 ft view before we dig in to each of the individual drug classes.
Stay tuned...
Do you want an HIV Cheat Sheet?
It’s hard to even call this a cheat “sheet,” as this sucker weighs in at 16 pages. But you could call these 16 pages “Basically everything you need to know about HIV pharmacotherapy.” It’s got renal/hepatic dosing adjustments, adverse effects and clinical pearls, brand/generic/abbreviation for every drug and combination product, preferred regimens for healthy adults, pediatrics, and pregnancy, opportunistic infection prophylaxis and treatment, adult and pediatric dosing tables, drug-drug interactions, drug-food interactions, and (seriously) a lot more.
This cheat sheet will save you a ton of time and frustration as you prep for the NAPLEX or any time you come across HIV in your practice.
It’s yours for only $19.