
How to Memorize Drug Side Effects (While Decreasing Your Study Time)
If you're a pharmacy preceptor (I am), or someone that spends a lot of time teaching pharmacology (I also am), then you've probably been asked some variation of the following question a hundred times:
"How can I possibly memorize and retain all of this drug information?!?"
And this is a totally legit question. I'm not the first person who has compared pharmacy school to "drinking from a fire hose" and I won't be the last. On one hand, thanks to the internet and online databases such as Micromedex and Lexicomp we basically carry the sum total of humanity's knowledge about pharmacy around in our pocket. But in a cruel twist of irony, this actually makes it more difficult to memorize the information we're studying...simply because we don't "have" to.
And rest assured, if you want to be the best (and most efficient) pharmacist you can be, there's a lot of stuff you need to commit to memory.
When I was a student asking the same "How do I remember all of this!?" question to my professors, the usual response was some variation of the immersion principle (i.e. study harder). This works for a bit but eventually, I found that I was getting diminishing returns. After a certain point, the extra time spent studying did not increase my retention (or my grades). And quite frankly, it took too damn long.
I was spending so much extra time staring at a textbook or lecture slides with no idea what I should be focusing on. I was hoping that if I could only spend "enough" time studying that the knowledge would magically burn itself in my brain.
Spoiler alert: That didn't happen.
So I experimented and came across the following process. I'm going to focus specifically on drug side effects in this article (because it is easier to understand if I speak in specifics and not in generalities), but this same approach can be applied to any area of studying.
The inside of Brandon's Pharmacy Brain. (Image)
This article is also a sneak peak into how my brain works with regards to pharmacy. These techniques are how I separate the wheat from the chaff; the important from the unimportant. I use these "learning by deconstruction" techniques, to create the articles and cheat sheets that are the core of tl;dr pharmacy.
These techniques are what got me through pharmacy school (not to mention the NAPLEX, MPJE and BCPS exams). If you apply them correctly, you'll retain more information in your study sessions without increasing the amount of time spent studying.
In fact, you'll likely decrease your study time. Once I started studying smarter, my "time in the trenches" decreased by at least an hour or two per week. Unfortunately, I didn't have the foresight to track before and after results, so you'll have to take me at my word.
Or better yet, run your own (n=1) experiment. Modify my system below to something that works for you and reap the rewards of "thoughtful" studying.
Learning by Deconstruction for Pharmacists
Alright, so again, for the purposes of this article let's focus on side effects.
I start by breaking down how side effects happen. What are the causes? I use a framework that I borrowed (read: stole) from toxicology to deconstruct the general category of "side effects" into its individual parts.
In essence, I'm using the engineering principle of deconstruction. It's almost like working backwards from the end to the beginning. The best way to learn how the engine in your car works is to take it apart and then put it back together. You start with the finished product, then separate it out to its individual components, then bring it all back together.
There's an excellent book called "The Art of Learning" written by Josh Waitzkin (for some random trivia, the author is who the movie "Searching for Bobby Fischer" was based on). In the book, he talks about how he was able to learn chess so quickly and effectively. His strategy was to begin with the end game.
Most players practice chess by learning opening moves that gain them control of the board. Josh Waitzkin did the opposite and started with the finale. He learned how to put the opponent in checkmate with any and every piece on the board. Then worked backwards to learn how to get into those end-game situations (which he'd mastered by now). It was like locking in a choke hold against an opponent in a UFC match. Your opponent may have controlled the last 3 rounds, but if you can lock them up in a strong choke hold it's game over. No matter how your chess match against Josh Waitzkin played out up to this point, eventually you found yourself in a situation where he knew how to lock you up in a choke hold (i.e. checkmate).
Anyway, back to pharmacy. Start with the end point of "adverse drug reaction" or "side effect," and work backwards to see the possibilities of how to get there. If you want to get really specific, you can try to envision test questions while you're studying. Work backward from possible test questions that might arise with the material you're studying.
In general, there are 4 main "causes" of drug toxicity:
Mechanism-Based (you'll often see these broken down into "On-Target" and "Off-Target" effects)
Toxic metabolites
Immune/hypersensitivity reaction to the drug
Idiosyncratic reactions
Let's look at each category separately.
1. Mechanism-Based
The first step is to understand the pharmacology of the drug itself.
This is absolutely critical.
For any given drug, the majority of its side effects are usually some extension of its mechanism of action. It might be the drug working "too well" or it might be the drug binding to the incorrect receptor (or even to the correct receptor in the wrong tissue).
If you truly learn pharmacology (and the related pathophysiology), then "memorizing" side effects is easy. It almost becomes unnecessary because you can use reason to figure out most potential side effects.
Yes, this is the same thing your professors have been telling you all throughout pharmacy school. And yes, it's true.
Mechanism-based side effects are further broken down into "on-target" and "off-target" effects. Off-target effects are exactly what they sound like. It's a drug binding to the wrong receptor (i.e. off target). On-target effects are categorized by where they occur (either the intended tissue or in an unintended tissue).
Set your eyes to "peep," and check out this picture to visualize what I'm talking about:

Let's plug in some familiar examples to illustrate the difference between on and off target.
A "classic" side effect of non-selective beta blockers (such as propranolol) is asthma exacerbation. This is an on-target effect because beta receptors are being appropriately blocked...but it's in an unintended tissue (the lungs instead of the heart).
Another calling card of beta blocker therapy is bradycardia...which is another on-target effect. This time, however, it's in the intended tissue.
For off-target effects, let's look at diphenhydramine. It's "supposed" to bind to H1 receptors, but many of its side effects stem from the fact that it also binds to (and blocks) cholinergic receptors. This leads to the classic anticholinergic effects such as dry mouth and urinary retention.
Alright, so enough with the science lesson. How do you actually memorize all of this?
Mechanism-based side effects usually extend to the entire class of drugs. You might learn that lisinopril can cause a dry, hacking cough. By learning the mechanism of that reaction (bradykinin build up secondary to ACE inhibition), you can now reason that every ACE inhibitor may cause a dry hacking cough. It's a class-wide side effect.
Another example is how all NRTIs can cause both lactic acidosis and hepatic steatosis via mitochondrial toxicity. Some individual drugs in the class may have a higher likelihood of lactic acidosis, but the potential risk exists for all of them.
So here's the take home point: You can learn mechanism-based side effects "once" for one drug, and you now know it for all other drugs in the same class. Make yourself a note card (or similar list) of on and off-target effects. And don't throw them away after you've taken the test for that module. They will come up again, I promise (even if only on the NAPLEX). Don't waste time re-writing out a bunch of notes you've already written up. Consider your drug study notes a list that evolves over your practice career. You add to it, take away from it, and modify it as necessary.
This forces you to re-review your notes every time you're looking for a specific piece of information and helps you connect the dots of the big picture.
2. Toxic Metabolites
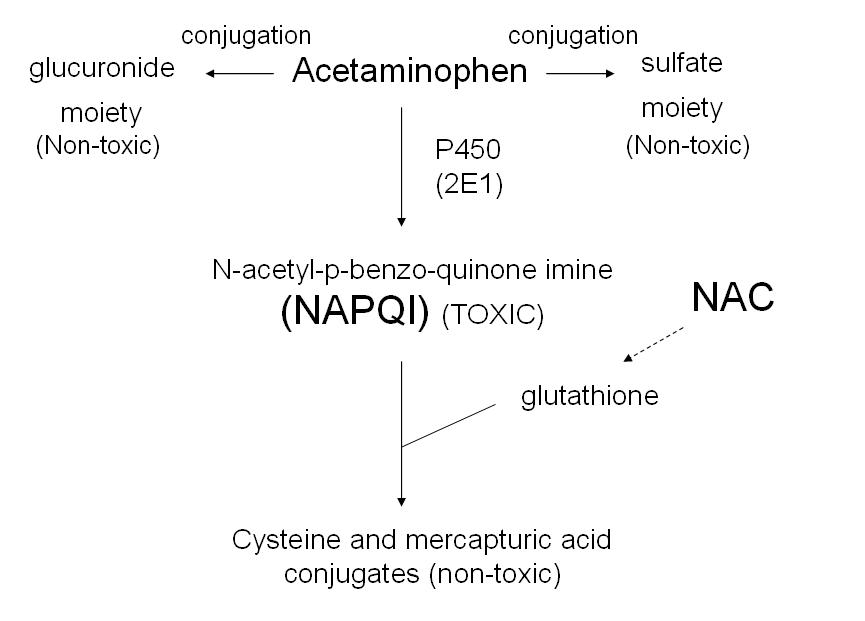
Another kind of side effect is due to toxic metabolites. These are byproducts of the metabolism of a parent drug that wreak havoc in your body. An example you're likely familiar with is N-acetyl-p-benzoquinone imine (NAPQI): the liver-destroying metabolic product of acetaminophen.
As a point of caution, I would not include active metabolites in this categorization (I'd classify active metabolites as causing mechanism-based toxicity because they're exerting the same pharmacologic effect as the parent drug).
There really aren't that many toxic metabolites that we have to deal with on a frequent basis in medicine. As you come across them in your studies, keep a list of them on a notecard and review it periodically. To really up your game, I recommend including the treatment or medical intervention for dealing with the toxic metabolite at hand (such as N-acetylcysteine for NAPQI).
3. Immune/Hypersensitivity Reactions
Sometimes you take a drug, and your body and immune system just goes ape shit on you. That's an immune reaction. Immune reactions to drugs are rare, but can be severe (ranging from a rash to hives to SJS to anaphylaxis) when they do occur.
There is a theoretic risk of any drug causing hypersensitivity, but you'll make the memorization process a lot easier on yourself if you single out the most common offenders. Focus your learning on the drugs most likely to cause an allergic reaction, and build out from there.
Here again, it's best to take a class-wide approach instead of focusing on individual agents (at least at first). I recommend making a list of drug classes that commonly cause immune reactions. For example, my own list includes penicillins, sulfa drugs, taxanes, and pretty much every monoclonal antibody.
Of course I'll include individual drugs too, especially if they're particularly noteworthy. Daratumumab, a monoclonal antibody used for multiple myeloma has a risk of infusion reaction that hovers around 50%. Additionally, I include drugs where we might test for human leukocyte antigen (HLA). Drugs like abacavir (HLA-B*5701) and carbamazepine (HLA-B*1502) have a very high risk of an immune reaction if given to individuals positive for the respective HLA.
4. Idiosyncratic Reactions
Idiosyncratic reactions are adverse events that don't fit into one of the categories above. For these little buggers, I find (again) that the best practice is to group drugs together that can cause a certain reaction.
For example, you might make a list of drugs that can prolong QTc interval (fluoroquinolones, macrolides, antipsychotics, 5-HT3 antagonists, etc...).
Of course, you don't just have to stick with idiosyncratic reactions. You can also make a list of (for example) drugs that can cause hyperkalemia (ACE inhibitors, ARBs, Aldosterone antagonists, aliskiren, heparin, SMT/TMP, etc...). You can do this for any side effect you can think of.
These drugs don't necessarily need to be in the same class. In fact, I think it's best if you throw in any drug from any class that applies. You could, for example, keep a running list of QTc prolonging drugs throughout school.

This serves a few purposes. First (and most importantly), it forces you to connect the dots. We learn things in a modular format in pharmacy school. It's easy to "learn and dump" the information as you go from test to test. With the rate that material is thrown at you during school, this is the option that most of us take (even if unintentionally). But the learn and dump process doesn't show you the forest for the trees. You miss out on how connected and similar medicine can be.
Having a list of drugs grouped together by side effect forces you to make some of those connections (and it allows you to be mindful of synergistic drug-drug interactions). You might be in an infectious disease module and you'll remember that linezolid has an interaction with the paroxetine that the patient in your test question takes for PTSD.
And secondly, every time you add something to one of your side effect lists, you'll naturally review the other drugs already on the list. This repetition is crucial and will help strengthen your drug info foundation.
Are you starting to notice a trend here? A large part of my memorization process is grouping "like with like." I make lists of drugs with similar traits or side effects...even if they're not in the same class or in the same therapeutic area. And the natural byproduct of this is that I see memorable connections between drugs that you might miss if you're going the module-to-module learn and dump route.
Useful Pharmacology/Therapeutics Memorization Tricks
Alright, so we've started with the end result (the adverse drug reaction). Then we broke that down into the 4 types of adverse drug reaction. Then we broke that down into individual examples (by mechanism) of drug toxicities.
This reverse engineering approach keeps you grounded in remembering the clinical applications of what you're learning. Google SJS/TEN just once (don't click on that link if you're squeamish), and you'll never forget what the implications of a hypersensitivity reaction can look like. And you'll remember that abacavir can cause that awful mess of a condition if you don't do an HLA test.
And we could stop there, and call it a wrap.
But then this wouldn't be a tl;dr pharmacy post.
So let's talk about some other useful memorization tricks to help shave hours off of your study time and get your grade over the hump.
One of my favorite "study hacks" is to memorize the exceptions to a rule. An example here is the renal dosing of antibiotics. There are only a small handful of commonly used antibiotics that don't require a renal adjustment. The "rule" here then, is to monitor kidney function for every antibiotic. Then, you can make a list of exceptions to the rule.
It's a hell of a lot easier to memorize these few outliers than it is to try to remember the massive list every antibiotic that requires a renal adjustment. The applications of this technique are practically endless. There's a ton of examples of drugs that are "exceptions to the rule." For example:
Abacavir is the only NRTI that does not require a renal adjustment
Ethambutol is the only drug in the RIPE regimen for tuberculosis that does not cause liver damage
Captopril is the only ACE inhibitor dosed 3 times daily (and is the only one used in hypertensive urgencies)
As you study a new topic (or review an old topic), look for the outliers. Look for the areas where a given drug doesn't fit the mold of the rest of its class. And keep an ongoing list of these exceptions.
This is the stuff that test questions are made of.
Another tip is to incorporate a (less lame) version of the immersion principle. The immersion principle doesn't mean you have to spend your life in a library quietly contemplating the mysteries of Pharm chem. It just means you have to be genuinely interested in (and spend a lot of time thinking about) a topic.
So find ways to incorporate what you're studying into your life. Make jokes about it. Talk about it with your friends. Tell funny stories about your experiences. You might come across as a little nerdy to an outsider but trust me this works (and don't worry, this is a safe and judgement free zone).
I still remember first learning about Revatio (the brand name for sildenafil used for pulmonary hypertension) because one of my classmates told us a story about how she overheard a man on the street trying to sell his "20 mg Viagra tablets." The powers of story and humor can leave a lasting impression.
But wait...there's more!
I didn't realize I was using them at the time, but during pharmacy school I used several cognitive "tricks" that help aid memorization when I was studying. Chances are, you might use at least one of them too (though you might not realize that it has a name).
The two tricks that worked for me were making personal associations with drugs and placing post-it notes all over my apartment. It was only after completing residency that I found out that there are well-known cognitive principles behind both of these (the Baker-baker paradox for making associations, and the Method of loci for my post-it notes).
To break down (quickly) how they work...
The essence of the Baker-baker paradox is that it is easier for you to remember that someone is a baker (their profession, or what they do for a living) than it is to remember that their last name is Baker. Think back on your own experiences with strangers you've met at a party or at the airport, and you'll probably find that it's true.
How I (unknowingly) applied this is that I "personified" the mechanism of action of drugs. I made up metaphors to describe how they worked and/or caused toxicity. For example, I might envision amphotericin B punching a hole in the nephron with a big spike...leading to the loss of potassium and magnesium (this turns out to be not too far from the truth).
18 oxen = a heck of a lot of folate. (Image)
In a less perfect analogy, I've always envisioned methotrexate as getting both it's efficacy and it's toxicity profile from the fact it "robs" the cell of folate. I have no idea why, but I've always thought of getting robbed while playing the Oregon Trail (I think I was playing a classic version of Oregon Trail during study breaks on my oncology module).
It's not a great analogy, because methotrexate stops you from producing folate more so than it depletes your folate...but it has nonetheless always worked for me (and I never forget to look for folic acid on the med profile of every patient taking methotrexate that I come across).
As for the Method of loci, it basically states that you can remember things if you associate them with a familiar environment. World Memory Championship contestants (yes, that's a thing) use this technique to memorize the order of an entire deck of cards in about 30 seconds.
I wasn't quite that extreme, but I did remember the exact location in my apartment of the post-it note that contained the information I needed for a test question. I even knew the spatial layout of my notes, and that the factoid being tested was in the upper right corner of my notebook. It was kind of eerie, I'm not gonna lie.
To give you an idea of how powerful this can be, I still remember the brand name for rifapentine (Priftin), that it is dosed weekly for latent TB infection, and that it's generally avoided for active TB...all because it was on a yellow post-it note on my refrigerator door.
I have not encountered (or even thought about) rifapentine since the infectious disease test I took in a therapeutics module 5 years ago.
Conclusion
Again, I should reiterate that you can use these study techniques for a whole lot of stuff besides side effects. Experiment with them, and find what works for you (and discard the rest). My system may not be for everyone, but it shaved hours off my study time and (in my opinion) actually increased my understanding of the material.
I hope these techniques will be as useful to you as they have been to me.